Hormones
Why Diets Stop Working After 40: It's Not a Fat Problem, It's a Muscle Problem
1 June 2026 · By Dr. B.J. Huber · 16 min read
You aren’t eating more than before. You aren’t moving less. But suddenly there is a new pad at your waist, the jeans button no longer closes properly. You try the same diet that always worked in your thirties. Two weeks fewer carbs, a bit more jogging. Nothing happens. Maybe you lose two kilos that are back within three weeks.
There is a reason for that, and it has almost nothing to do with discipline.
In perimenopause your metabolism shifts in a way that breaks classic diet logic. Your body moves from a phase where oestrogen kept muscle, insulin sensitivity and fat distribution stable into a phase where all three are simultaneously disrupted. The old diet no longer works because the problem has become a different one.
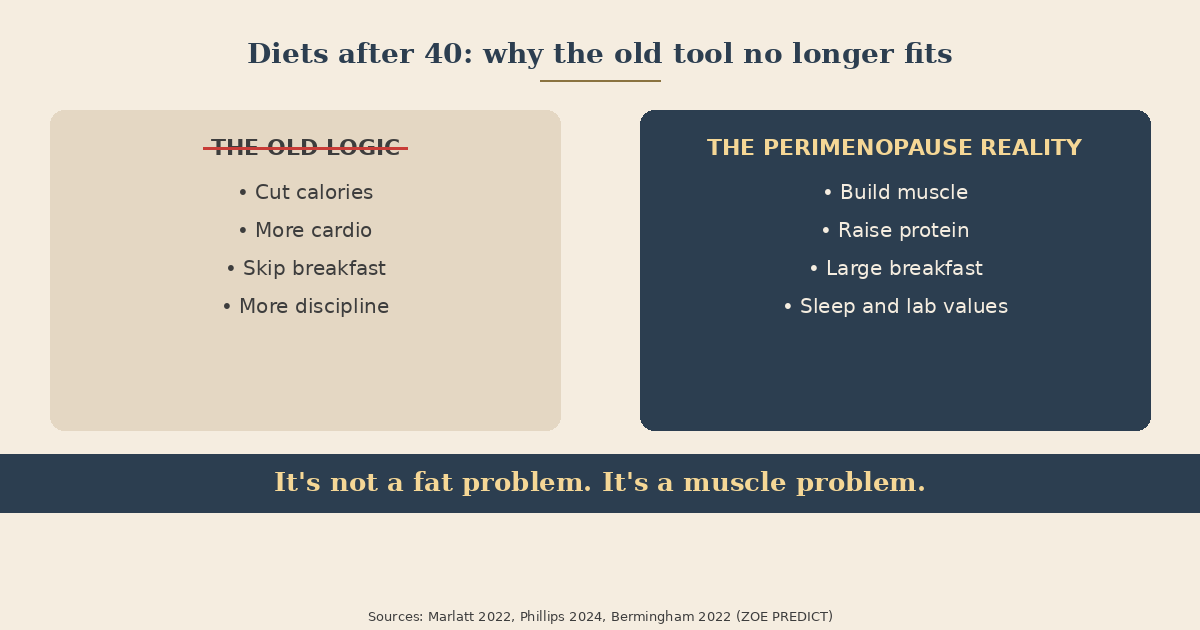
The most important reframe this article works with: It’s not a fat problem, it’s a muscle problem. That changes what you do as soon as you understand it.
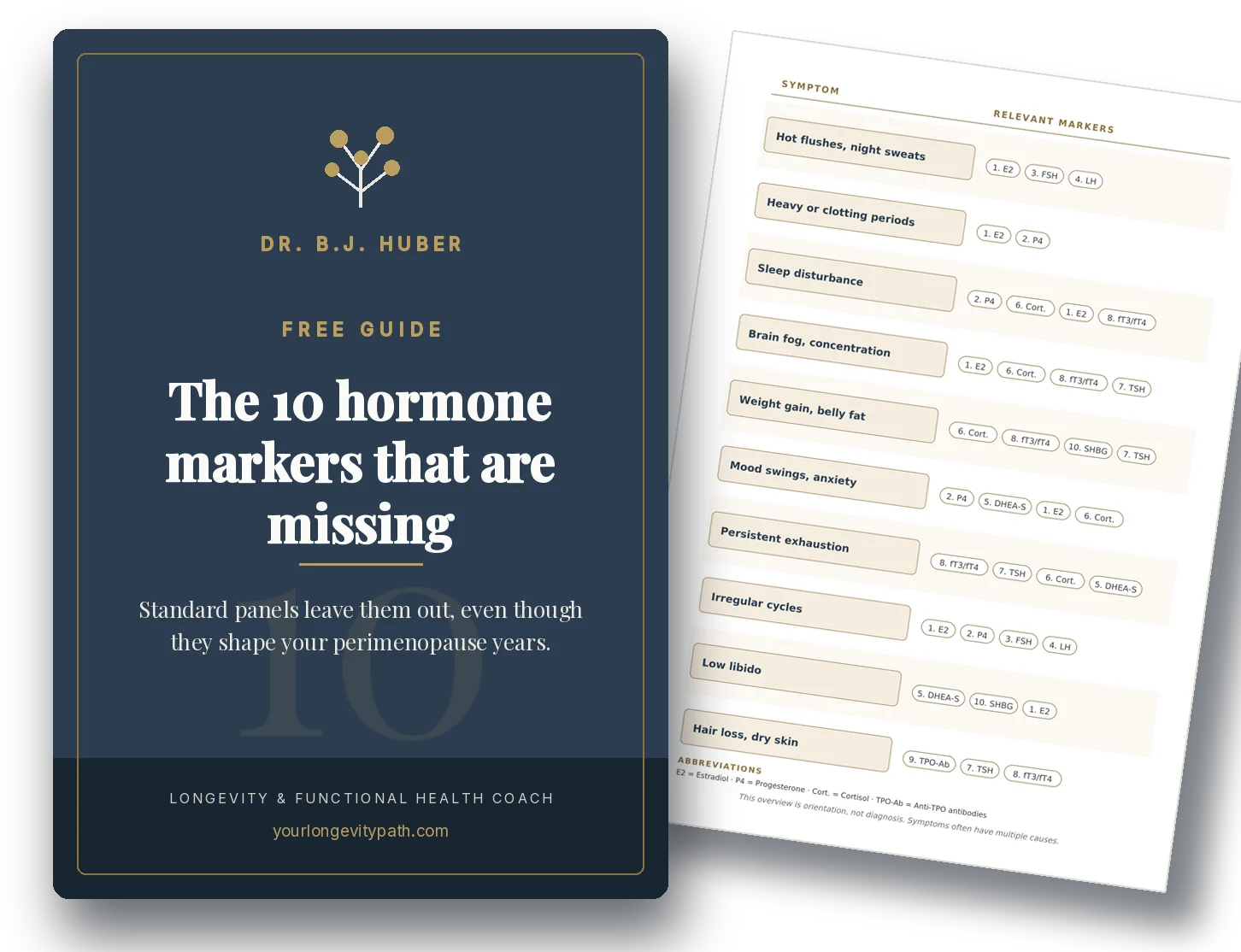
- A large share of women in perimenopause gain weight at the waist without eating more. The main mechanism lies in a creeping insulin resistance and a loss of muscle mass, not primarily in the calorie balance.
- Skeletal muscle absorbs about 80 per cent of postprandial glucose. Less muscle means less buffering, higher glucose spikes, more storage as fat.
- In the age-matched ZOE PREDICT subgroup, postmenopausal women showed a 42 per cent higher postprandial glucose load (area under the curve over two hours) compared with premenopausal women (Bermingham et al., 2022).
- The single most effective lever is muscle gain plus adequate protein, not eating less. Hormone therapy and GLP-1 medications are medical topics with clear pros and cons.
Why doesn’t your old diet work anymore?
In perimenopause, oestrogen falls, which directly regulates the insulin sensitivity of your muscle, your liver and your blood vessels. At the same time you slowly lose muscle mass, and fat redistributes. A classic calorie-restriction diet often amplifies this shift rather than resolving it.
The feeling that “my body has become a different one” has a real biological basis. SWAN data show that the change in body composition is coupled to the menopause transition rather than to chronological age (Marlatt et al., 2022). Specifically: lean mass declines measurably faster from the last menstruation onward, visceral fat (fat surrounding the internal organs) rises faster. The same woman in the same year of life changes differently depending on where she is in the hormonal transition.
Classic diets rely primarily on calorie restriction. In perimenopause you lose disproportionately muscle rather than fat, because muscle responds less robustly to the protein anabolic signal. Less muscle means less resting metabolic activity, less glucose buffering after every meal and a faster yo-yo rebound. You have used the same tool for a different problem.
What shifts first in perimenopause — oestrogen or FSH?
Both shift, but not at the same time. Follicle-stimulating hormone (FSH) often rises years before the clear oestrogen drop, and it has independent effects on fat distribution and bone. That explains why many women feel symptoms in early perimenopause even though their oestradiol still looks “normal”.
Most of the hard metabolic data found in textbooks comes from postmenopausal studies. That distorts the picture, because women feel the symptoms already in the peri phase. FSH is the most important explanatory building block here.
A mechanistic study from the Mount Sinai group showed in a mouse model that blocking FSH signalling markedly reduces visceral fat and induces brown thermogenic adipose tissue (Liu et al., 2017). For honest framing: this is a preclinical study, not an approved therapy in humans. What the study does establish conceptually is that FSH is an independent driver of fat distribution, not merely a side signal of oestrogen withdrawal. Clinical FSH antibody studies are in preparation but not a practical tool today.
Practical consequence: If you are gaining belly fat in early perimenopause even though your values still look “normal”, that is not imagined. The hormonal transition begins biochemically earlier than a standard hormone panel makes it visible.
It’s not a fat problem, it’s a muscle problem
Your skeletal muscle is by far the largest glucose sink in your body. After a meal, your muscles absorb about 80 per cent of the glucose from your blood, controlled via insulin signalling and a transporter called GLUT4 that acts like a gate between blood and muscle cell. The less muscle you have, and the less insulin-sensitive it is, the higher the spikes, and the more glucose gets stored instead in liver and abdominal fat (DeFronzo & Tripathy, 2009).
Oestrogen supports this mechanism at several points. It promotes mitochondrial respiration in muscle, the insulin signalling cascade, and the readiness of muscle cells to bring GLUT4 to the surface (Hevener et al., 2020). When oestrogen falls, all of these steps weaken.
On top of that comes a second effect that is often underestimated: anabolic resistance. Muscle protein synthesis responds less robustly to protein in perimenopause. Simplified: a 30-year-old woman gets a solid building response from 20 g of protein per meal. A 50-year-old needs closer to 30 to 40 g for the same response, and she needs regular resistance training stimuli to let the signal through at all (Deane et al., 2024).
What does that mean in practice?
- Eating less alone reduces muscle more than fat. You sabotage exactly the tissue that maintains your metabolism.
- More muscle = more glucose buffer = better readings. Even 1 to 2 kilos more lean mass can measurably improve the postprandial glucose response.
- Strength training is not “also nice to have”, it’s the dominant lever. Cardio complements; strength is the base.
This is the reframe this article carries. The moment you define muscle gain as the goal rather than weight loss, your nutrition, training, sleep planning and even the lab markers you check shift.
Why does the fat land at the waist now?
Oestrogen keeps fat preferentially in “safe” depots: hip, glute, thigh (the classic pear pattern). When oestrogen falls, fat is increasingly stored viscerally, that is, around the internal organs in the abdomen. Visceral fat is metabolically active, secretes inflammatory messengers, and amplifies insulin resistance further.
Marlatt et al. (2022) in their review of body composition across the menopause transition show: visceral adiposity typically rises by 10 to 20 per cent across the transition while subcutaneous fat only rises moderately. The acceleration begins in late perimenopause and stabilises about two years after the last menstruation. So it is a phase, not a permanent state, but it leaves a different starting point than premenopausal.
Mechanistically this is explained from three angles:
- Oestrogen protects subcutaneous storage. When it falls, fat “leaks” into the visceral depot.
- FSH rises in parallel. As described above, FSH has independent effects on fat distribution.
- Fat ends up where it doesn’t belong. Lipids are increasingly stored in liver and muscle, which further blunts insulin signalling there (in technical terms: ectopic lipid deposition with lipotoxicity).
Practical implication: in perimenopause, waist circumference is a more important risk marker than body weight. A waist circumference above 88 cm in women is associated with notably increased insulin resistance and cardiovascular risk, even at “normal” BMI.
How does your glucose response change measurably?
The largest study on this comes from ZOE PREDICT, which compared meal-related glucose responses by continuous glucose monitoring (CGM) in around 1,000 women. In the age-matched subgroup, postmenopausal women showed a 42 per cent higher postprandial glucose load over two hours, measured as area under the glucose curve. The actual glucose peak was only about 4 per cent higher, but the return to baseline took notably longer (Bermingham et al., 2022).
Additional shifts in the age-matched comparison:
- Fasting glucose +6 per cent
- HbA1c +5 per cent
- Inflammation marker GlycA +4 per cent
- Sugar consumption +12 per cent
- Sleep quality −12 per cent
The most important message of this study is not “postmenopausal = bad metabolism”. It is much more specific: individual glucose responses scatter enormously. Two women of the same age, the same weight and the same meal can show entirely different glucose spikes. Statistical analyses of the ZOE data suggest that part of this scatter is explained by dietary patterns and the composition of the gut microbiome. That argues against any “one diet fits all” logic and for a personalised baseline.
A practical CGM trial (two to four weeks, medically prescribed) can be a learning tool: which meal drives your glucose, which keeps it stable, how a walk after dinner shifts the curve. Honestly: in women with a history of eating disorders or strong hyperfocus tendencies, CGM can amplify symptoms. The tool is then not the right one.
How are sleep, stress and the gut microbiome connected to your insulin level?
Sleep, cortisol and the gut microbiome are three amplifiers that have to appear in any serious strategy for insulin sensitivity. In perimenopause they are additionally destabilised.
Sleep. Zuraikat et al. (2024) showed in a crossover trial in 36 women that six weeks of mild sleep restriction (one-and-a-half hours less per night) measurably worsened insulin sensitivity, and notably did so independent of changes in fat mass. The effect was more pronounced in postmenopausal than in premenopausal women. Important: it isn’t weight driving the deterioration here, it’s the sleep loss itself.
Sleep apnea. Postmenopausal risk for obstructive sleep apnea rises markedly because oestrogen and progesterone stabilise upper-airway muscle tone. Sleep apnea worsens insulin sensitivity independently of weight and is massively under-diagnosed in women. If you do not wake rested despite lifestyle adjustments, you belong in a sleep lab. The mechanisms I have laid out in detail in the sleep article.
Cortisol. Oestrogen dampens the HPA axis (the stress system). With oestrogen withdrawal the cortisol response becomes more reactive, the day curve often flatter, and evening cortisol falls more slowly. Chronically elevated cortisol drives the liver to release sugar into the blood on its own and promotes visceral fat storage. Stress regulation is no wellness add-on here, it is a direct metabolic lever.
Microbiome. ZOE data show that the composition of the gut bacteria explains part of the glucose variability. Fibre diversity, fermented foods and adequate plant variety make sense, with one important caveat: in perimenopause many women suddenly tolerate aggressive “30 plants a day” strategies less well. I have addressed this in more detail in the gut advice article.
Alcohol. A point that in practice often has the biggest leverage and is most easily underestimated. Alcohol directly worsens sleep quality (less REM), triggers nocturnal hot flashes, inhibits the liver’s overnight sugar production (with reactive hunger the next day) and promotes visceral fat storage via hepatic metabolism. Even one glass of wine per evening measurably makes a difference in perimenopause.
Why this isn’t “just” about weight
Insulin resistance in midlife is not primarily an aesthetic problem. It is a longevity marker. Elevated fasting insulin and rising HOMA-IR go together with higher risk of type-2 diabetes, cardiovascular events and cognitive decline.
A more recent research strand refers to insulin resistance in the brain as “type-3 diabetes”. Brain cells too depend on insulin signalling for glucose uptake and energy production. When this signalling blunts, cellular energy degrades exactly where you need clarity, memory and focus. That is one of the mechanistic links between midlife metabolic shifts and long-term dementia risk.
From a longevity perspective, insulin sensitivity is therefore one of the few levers that simultaneously influence heart, brain, bone and energy budget. Whoever invests here in midlife is building for decades.
What actually helps?
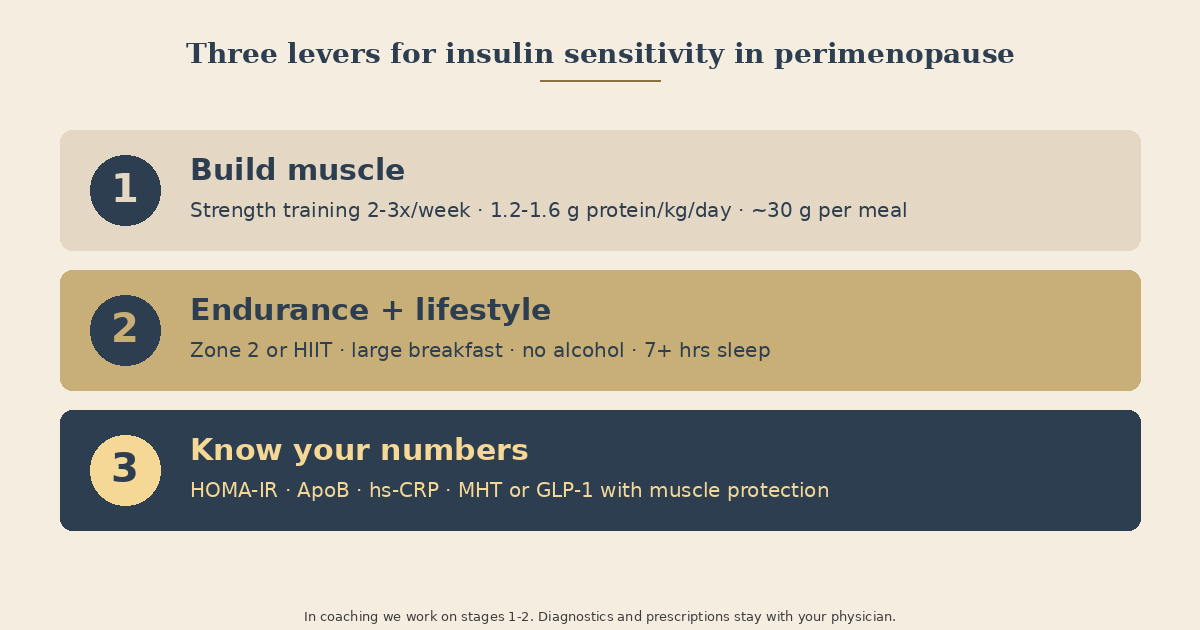
The honest answer: no single tool is the solution, but three levers consistently produce the largest effect in trials. These are the three levers we work on in coaching.
1. Build muscle. The dominant lever. Concretely:
- Strength training 2–3×/week, every major movement (squat, hinge, push, pull) with progressive load, 2–4 sets at moderate intensity (6–12 reps).
- Protein as a daily total: 1.2–1.6 g per kilogram body weight, distributed across 3–4 meals.
- Pragmatic per meal: around 30 g. Particularly important at breakfast, where many women eat only 10–15 g.
- Plant-based eating: tend to add a bit more total because plant protein has less leucine per gram.
- Creatine in monohydrate form (3–5 g daily) has improved muscle response to training in several studies in peri- and postmenopausal women (Smith-Ryan et al., 2025).
2. Endurance + lifestyle. The second layer that sharpens your energy machinery:
- Endurance: 2× per week in addition to strength training. Either zone 2 (45–60 minutes of brisk walking or cycling at a still-conversational pace) or short HIIT intervals (4×4 minutes at 85–95 % of maximum heart rate with active recovery). Both improve the energy plants of the muscles and the glucose gates at the cells (Bishop et al., 2019).
- Large breakfast, small dinner measurably reduces HOMA-IR at equal calories (Jakubowicz et al., 2013).
- Keep evening glycaemic load low: fewer fast carbs late, more protein and vegetables.
- Drop alcohol or reduce it markedly. Even one glass of wine per evening makes a measurable difference in perimenopause.
- Target over seven hours of sleep — a direct metabolic lever, not a wellness add-on.
3. Know your numbers, work with your physician. Before stacking supplements or programmes, an honest baseline is worth it. Fasting insulin, HbA1c and HOMA-IR reveal insulin resistance years before glucose does. ApoB for vascular risk, hs-CRP for silent inflammation. Which markers matter particularly in perimenopause and how to interpret them I have summarised in the blood test article.
When does medical guidance make sense?
Three scenarios go beyond what coaching can cover:
Menopausal hormone therapy (MHT). For severe hot flashes, night sweats or sleep symptoms, MHT is an evidence-based option. A meta-analysis of 17 randomised trials in nearly 5,800 non-diabetic postmenopausal women showed that MHT significantly lowers insulin resistance, with a larger effect under oestrogen alone than under oestrogen plus progestogen (Li et al., 2025).
For honest framing: indication for MHT is symptom control, not “insulin resistance therapy”. The metabolic improvement is a real bonus, not a standalone prescribing reason. Indication, route (transdermal vs oral) and dose stay with your gynaecologist.
GLP-1 agonists (semaglutide, tirzepatide). These medications produce striking weight loss in women with obesity.
- What they can do: In the SURMOUNT study with tirzepatide, average weight loss in adults with obesity exceeded 20 per cent, somewhat higher in the women’s subgroup than in men. A retrospective Mayo Clinic cohort additionally suggested that women on tirzepatide plus MHT lost more weight than those on tirzepatide alone. Important framing: that is an association, not causal proof (n=120, prospective studies pending).
- The catch: Under GLP-1 therapy, lean mass accounts for a meaningful fraction of the weight lost. In the SURMOUNT substudy that was around 25 per cent, and more under semaglutide.
- The consequence: Anyone using GLP-1 without strength training and adequate protein loses muscle she will not easily regain after the therapy. In perimenopause, where anabolic resistance is already higher, this is particularly critical. Strength training and protein are not optional under GLP-1.
In coaching we work on points 1 and 2: the daily building task, the connection between strength training, protein, sleep, nutrition and stress regulation. Prescriptions and diagnostics remain medical.
Bottom line
Diets stop working after 40 because the problem has changed. The old logic “eat less, move more” is an answer to too much fat. In perimenopause the answer is: more muscle, better insulin signal, smarter distribution of carbohydrates and sleep.
What you do shifts fundamentally with that. Instead of counting calories you plan protein distribution. Instead of jogging you go to the rack. Instead of skipping breakfast you make it the largest meal of the day. Instead of looking for a “menopause diet” you build muscle and give your body back the tools it has lost in perimenopause.
If you would like to look at your own metabolic picture concretely, you are welcome to a free initial consultation — together we can think through which lever is the right starting point for you.
Scientific Sources
-
Bermingham KM et al. Menopause is associated with postprandial metabolism, metabolic health and lifestyle: The ZOE PREDICT study. eBioMedicine. 2022;85:104303. doi:10.1016/j.ebiom.2022.104303
-
Bishop DJ et al. High-intensity exercise and mitochondrial biogenesis: current controversies and future research directions. Physiology (Bethesda). 2019;34(1):56–70. doi:10.1152/physiol.00038.2018
-
Deane CS, Cox J, Atherton PJ. Critical variables regulating age-related anabolic responses to protein nutrition in skeletal muscle. Front Nutr. 2024;11:1419229. doi:10.3389/fnut.2024.1419229
-
DeFronzo RA, Tripathy D. Skeletal Muscle Insulin Resistance Is the Primary Defect in Type 2 Diabetes. Diabetes Care. 2009;32(Suppl 2):S157–S163. doi:10.2337/dc09-S302
-
Hevener AL et al. The Impact of Skeletal Muscle ERα on Mitochondrial Function and Metabolic Health. Endocrinology. 2020;161(2):bqz017. PMC7017798
-
Jakubowicz D et al. High caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity. 2013;21(12):2504–2512.
-
Li T, Jiang NS, Kaskey J, Schnatz PF, Nudy M. Hormone therapy and insulin resistance in non-diabetic postmenopausal women: a systematic review and meta-analysis. Climacteric. 2025;28(6):673–681. doi:10.1080/13697137.2025.2509844
-
Liu P et al. Blocking FSH induces thermogenic adipose tissue and reduces body fat. Nature. 2017;546:107–112. (Preclinical mouse study)
-
Marlatt KL et al. Body composition and cardiometabolic health across the menopause transition. Obesity. 2022;30(1):14–27. doi:10.1002/oby.23289
-
Smith-Ryan AE et al. Creatine in women’s health: bridging the gap from menstruation through pregnancy to menopause. J Int Soc Sports Nutr. 2025;22(1):2502094. doi:10.1080/15502783.2025.2502094
-
Zuraikat FM et al. Chronic Insufficient Sleep in Women Impairs Insulin Sensitivity Independent of Adiposity Changes: Results of a Randomized Trial. Diabetes Care. 2024;47:117–125. PMID:37955852
Why am I suddenly gaining weight in menopause without changing anything?
In perimenopause, oestrogen falls and follicle-stimulating hormone (FSH) rises. Both shifts move fat from the hip and glute region into the abdomen and reduce the insulin sensitivity of your muscle. The same meal now produces a longer glucose load, with more storage as fat and less buffering by muscle.
Why don't diets work the way they used to after 40?
Classic diets rely on calorie reduction. In perimenopause you lose disproportionately muscle rather than fat, because anabolic resistance increases. Less muscle means less glucose buffering, slower metabolism, and faster regain. The lever is muscle gain, not less food.
Does strength training really help against the 'menopause belly'?
Yes. Skeletal muscle absorbs about 80 per cent of postprandial glucose. More muscle means more glucose buffer, higher insulin sensitivity and less visceral fat. In studies of postmenopausal women, strength training two to three times per week measurably improves insulin sensitivity and body composition.
Which blood tests are worth checking?
Fasting insulin and HbA1c often reveal insulin resistance years before glucose does. HOMA-IR (calculated from both) is the most practical marker. Add ApoB for vascular risk and hs-CRP for silent inflammation. Which markers are particularly worthwhile in perimenopause I have laid out in a separate article.
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.