Hormones
3 Hormonal Axes No One Explains: Why Your Sleep Collapses in Perimenopause
30 May 2026 · By Dr. B.J. Huber · 13 min read
You wake up at 3 a.m., bolt upright, heart pounding. You are exhausted and wide awake at the same time. Two years ago you slept like a stone. Now you lie there, staring at the ceiling, asking what is wrong with you. People ask if you are stressed. You nod, because the real answer is more complicated. You feel like someone else.
In perimenopause, three biological systems your brain has been using for decades to power down at night collapse at the same time. Once you understand which axis is doing the heavy lifting for you, you also know where the lever is.
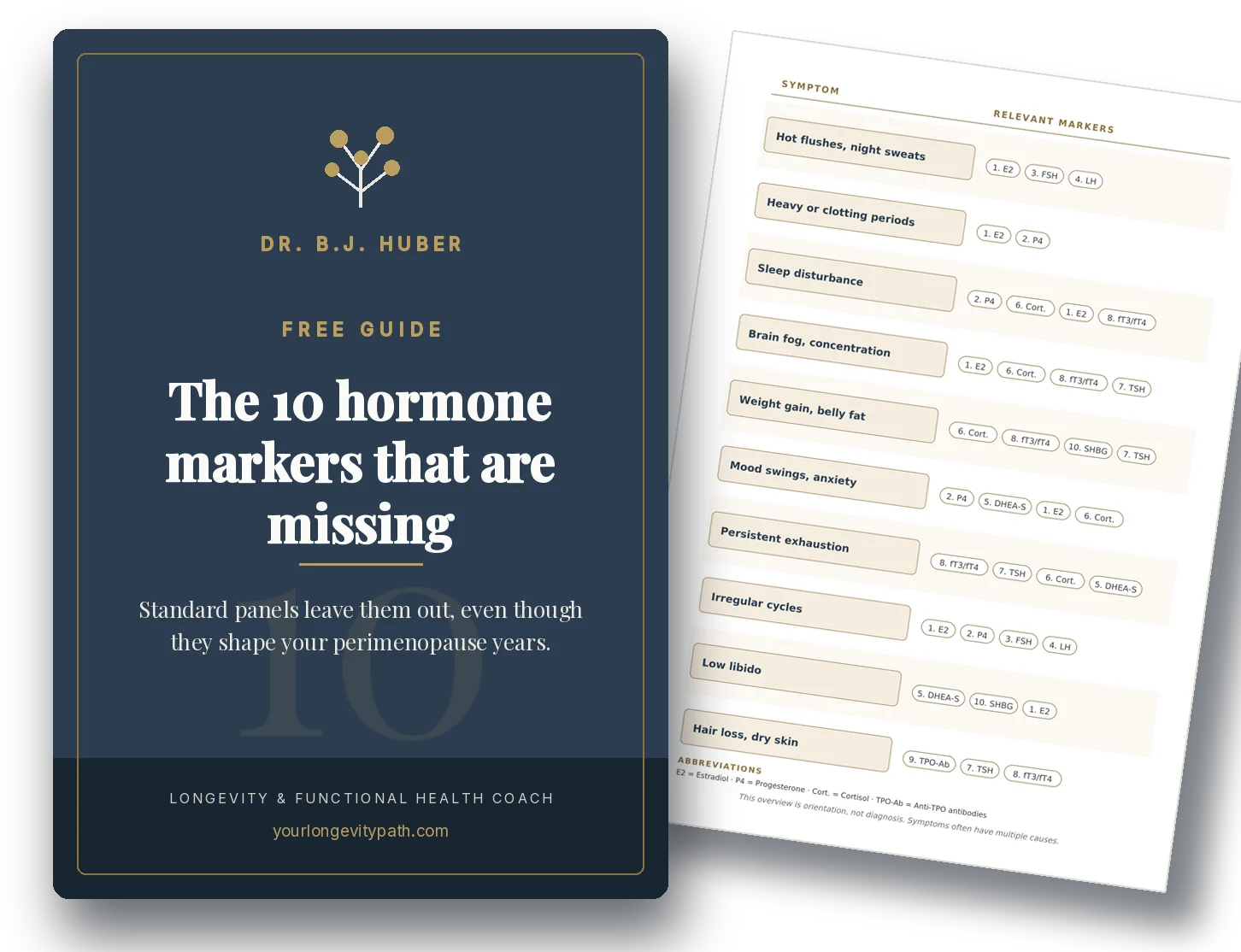
- Between 40 and 60 per cent of women develop new sleep-onset or sleep-maintenance problems in perimenopause. A meta-analysis of 37 studies in over 29,000 women shows a 50.8 per cent prevalence of poor sleep quality (Yu et al., 2024).
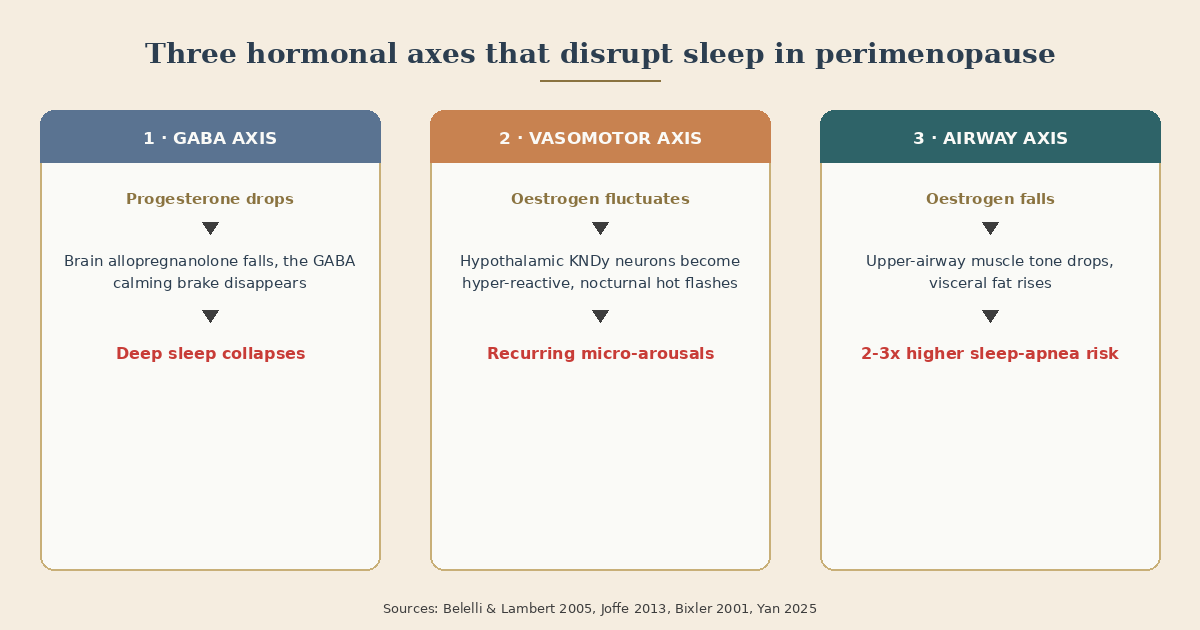
- Sleep drifts out of balance along three clearly separable axes: the loss of the body’s endogenous calming brake (GABA axis), nocturnal hot flashes from the hypothalamus (vasomotor axis), and a fading tone of the upper airway (airway axis).
- Persistent insomnia and short sleep duration in midlife raise cardiovascular risk by 70 to 75 per cent independent of classical risk factors (Thurston et al., 2024).
- Diagnostics and prescriptions stay with your physician. In coaching we work on the foundation: sleep architecture, lifestyle levers, and targeted micronutrients.
Why does sleep collapse precisely in perimenopause?
Perimenopause is not “just less oestrogen”. It is a phase of chaotic hormonal fluctuation across several years, during which three sleep systems lose stability in sequence. That is why the picture is so confusing for many women: first only trouble falling asleep, then night sweats, then suddenly daytime fatigue that no amount of sleep seems to repair.
The longitudinal data from the SWAN study (Study of Women’s Health Across the Nation) demonstrated in over 3,000 women that sleep complaints begin in early perimenopause and intensify in late perimenopause (Kravitz et al., 2008). A current meta-analysis spanning 37 studies and 29,284 women confirms it: 50.8 per cent report poor sleep quality, compared with roughly 30 per cent in premenopausal control groups (Yu et al., 2024).
That rules out “you’re simply getting older” as a sufficient explanation. The hormonal transition itself drives the difference. It works across three axes.
Axis 1: What does progesterone have to do with deep sleep?
Progesterone is converted in your brain into allopregnanolone. This compound activates a specific calming brake on your neurons, the same one benzodiazepines target, but without the tolerance or dependency. In the scientific literature these are referred to as the GABA receptors.
When progesterone drops, this endogenous deep-sleep switch drops with it. You wake more easily, sleep becomes shallower, the deep-sleep fraction shrinks.
Belelli and Lambert (2005) described the mechanism at the neuronal level. Caufriez et al. (2011) showed in a placebo-controlled study in postmenopausal women: 300 mg of oral micronised progesterone at bedtime measurably lengthened deep-sleep duration and reduced night-time wake periods, verified in the sleep lab. The later meta-analysis by Nolan et al. (2021) pooled this evidence. It showed a clear effect on sleep-onset latency; results were more heterogeneous for total sleep time and sleep efficiency.
This also explains why many women have sleep problems in early perimenopause, long before they lose meaningful amounts of oestrogen. The first anovulatory cycles no longer produce a second half of the cycle with high progesterone. The peak of your endogenous calming system disappears before hot flashes ever show up.
Oral micronised progesterone at bedtime is an evidence-based option within menopausal hormone therapy. Prescription and dose are clinical decisions.
Axis 2: Why does a hot flash pull you out of sleep at 3 a.m.?
Inside your hypothalamus sits a cluster of neurons that monitor your core body temperature. In perimenopause these neurons become hyper-reactive. They suddenly signal “you are too hot” even when you are not. Your body responds with sweating and skin flushing. In the literature this specialised cell group is called the KNDy neurons.
What matters for sleep: these hot flashes are tightly linked to nocturnal awakenings, but not in the way most women assume. Joffe et al. (2013) showed in a study of 20 women using a hormonally induced model that nocturnal hot flashes are objectively coupled to awakening phases. Bianchi et al. (2016) then went closer with polysomnography in a larger group (n = 28): around 66 per cent of nocturnal hot flashes occurred within five minutes of an awakening, with a large share immediately before or during the wake event. Often the hot flash followed the awakening rather than triggering it.
That shifts the model. The brain wakes up first; the hot flash follows. Both are driven by the same mechanism: a hyper-reactive hypothalamus that is missing its hormonal damping.
The new class of neurokinin-receptor antagonists targets exactly this. Fezolinetant (SKYLIGHT 1+2, Lederman et al., 2023) and elinzanetant (OASIS 1+2, Pinkerton et al., 2024) block NK3 signalling in the hypothalamus and measurably reduce nocturnal hot flashes. In the OASIS trials, sleep quality also improved directly — an effect that appears to extend beyond the simple reduction of hot flashes and suggests an additional action on sleep regulation.
Fezolinetant is approved in the EU as Veoza. Elinzanetant has been available in the US since October 2025 as Lynkuet. Both are prescription only and DACH reimbursement is still evolving.
Axis 3: Are you snoring, or are you just waking up “off”?
Oestrogen and progesterone help maintain muscle tone in your upper airway, particularly in the tongue muscle and the throat. At the same time, fat distribution shifts in perimenopause. Visceral fat (fat surrounding the internal organs) increases. Both changes raise the risk of obstructive sleep apnea, repeated brief pauses in breathing during sleep.
Bixler et al. (2001) documented in a population-based sample: 2.7 per cent of postmenopausal women without hormone therapy had moderate-to-severe sleep apnea, compared with 0.6 per cent of premenopausal women and 0.5 per cent of women on hormone therapy. Huang et al. (2018) showed additionally that surgical menopause (ovary removal) is an independent risk factor for sleep apnea, with effect sizes not explainable by BMI alone. Wang et al. (2025) confirm the independent effect of visceral fat.
The catch: women are massively under-diagnosed for sleep apnea. They snore more quietly, witnessed apneas are rarer (often because the partner does not notice), and they present primarily with insomnia, fatigue and low mood, rarely with the textbook “excessive daytime sleepiness” that guidelines describe.
If you do not wake up rested despite lifestyle adjustments, a cool bedroom and balanced micronutrients, you belong in a sleep lab. Even without loud snoring.
Why does sleep feel worse than the measurements show?
Many women in perimenopause feel like they “lay awake all night” while objective sleep duration is only mildly reduced. Sleep perception shifts. Lampio et al. (2021) followed women over ten years with polysomnography and subjective sleep diaries. Result: many of the objectively measurable changes are age-related and occur in both sexes. What changes measurably in perimenopause is the frequency of brief awakenings and the subjective sense of restoration.
That explains why you are not “wrongly” exhausted when your sleep-lab report shows “only” 20 minutes of wake time. The fragmentation, the brief awakenings and the loss of deep-sleep stages explain why six hours of sleep can feel like three.
Why this isn’t “just” about sleep quality: it’s about longevity
Poor sleep in midlife is not a comfort problem. It is a metabolic and cardiovascular problem with long-term consequences.
Thurston et al. (2024) demonstrated in 2,517 midlife women followed for up to 22 years that women with concurrent persistent insomnia AND short sleep duration had roughly a 75 per cent higher risk of cardiovascular events, independent of blood pressure, BMI and lipids. Short sleep alone, without clinical insomnia, raised the risk only modestly and to borderline significance. Zuraikat et al. (2024) showed in a crossover trial in 36 women that six weeks of mild sleep restriction (one-and-a-half hours less per night) measurably worsened insulin sensitivity, and notably did so independent of changes in fat mass. The effect was more pronounced in postmenopausal than in premenopausal women. Marlatt et al. (2022) confirmed the relationship between sleep quality and postmenopausal accumulation of visceral fat.
Sleep is therefore one of the largest and most under-appreciated longevity levers in perimenopause.
What actually helps — and what does not
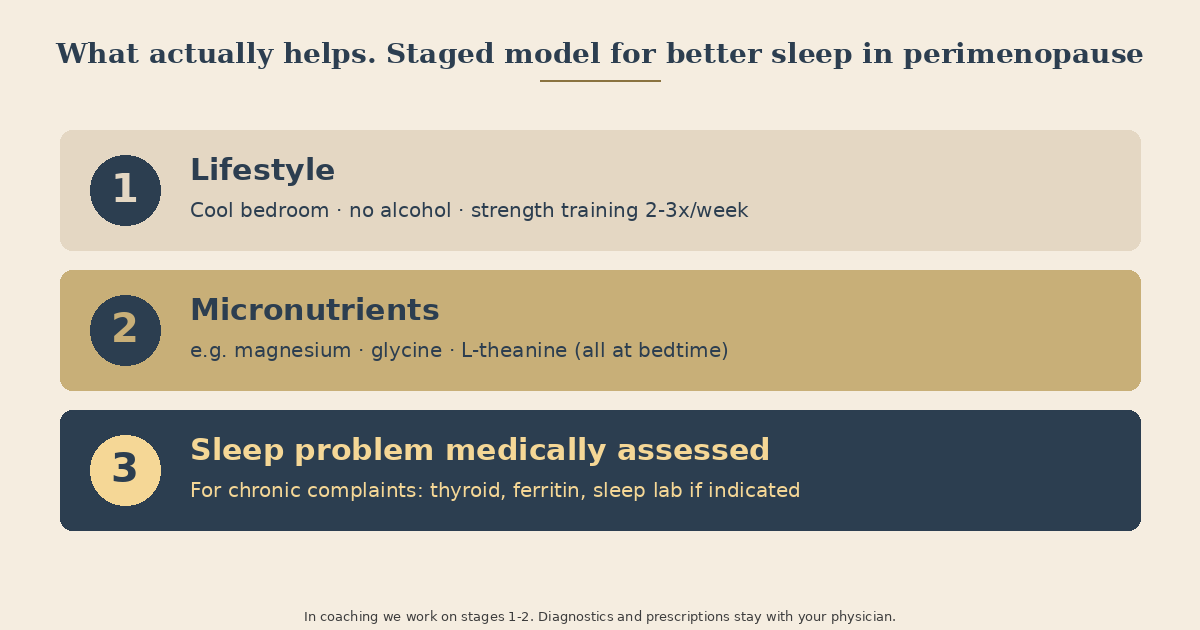
The honest answer: no single intervention covers all three axes. A staged approach makes sense.
1. Get your hormonal and metabolic picture first. Sleep problems in perimenopause often overlap with iron deficiency, thyroid shifts or insulin resistance. Which biomarkers actually matter in this phase, I have laid out in a separate article: Which blood tests really matter in perimenopause. Get the foundation right first; then build on top.
2. Lifestyle foundation. Consistent bed and wake times measurably shift your circadian rhythm. Keep the bedroom cool (17 to 19 degrees Celsius) so core body temperature can fall. Drop alcohol at least three hours before bed, ideally entirely. Even one glass of wine triggers more frequent nocturnal hot flashes and measurably reduces REM sleep. Keep glycaemic load low in the evening: late sugar peaks lead to reactive hypoglycaemia around 3 a.m., with adrenaline release and awakening. Strength training two to three times per week reduces vasomotor burden and improves subjective sleep quality in trials (Berin et al., 2019).
3. Micronutrients with evidence. Magnesium bisglycinate or magnesium L-threonate (200 to 400 mg at bedtime) improves subjective sleep quality in trials. Glycine (3 g at bedtime) shortens sleep-onset latency and improves subjective sleep quality. L-theanine (200 mg at bedtime) is anxiolytic and shortens time to fall asleep.
4. Hormonal therapy evaluated medically. For severe vasomotor symptoms or prominent perimenopausal insomnia, menopausal hormone therapy is an evidence-based option. Transdermal estradiol plus oral micronised progesterone at bedtime is first-line in most current guidelines because transdermal estradiol carries a more favourable thrombosis profile than oral oestrogen. Indication and dose belong with your gynaecologist.
When do the symptoms belong with a physician?
If sleep problems persist for more than four weeks, if you do not wake rested after eight hours in bed, if your partner observes breathing pauses, if you wake with leg restlessness, if mood deteriorates as well: this needs medical workup. Sleep problems in perimenopause are too often treated as depression before hormone status, thyroid, iron stores or sleep apnea have been ruled out. The order matters.
In coaching we work on what does not fit into a consultation: the daily foundation, sleep architecture, the connection between lifestyle, micronutrients and sleep.
Bottom line
Sleep in perimenopause rarely breaks for a single reason. Three hormonal axes shift at the same time: the GABA calming brake (progesterone axis), hypothalamic heat regulation (vasomotor axis), upper-airway tone (airway axis). Understanding which axis carries the most weight for you tells you where the lever is.
The good news: all three are modifiable. What does not work is “you just need to relax more”. What does work is a staged strategy that begins with a clear hormonal and metabolic picture and follows the evidence.
If you would like to look at your own sleep picture concretely, you are welcome to a free initial consultation — together we can think through which lever is the right starting point for you.
Scientific Sources
-
Belelli D, Lambert JJ. Neurosteroids: endogenous regulators of the GABA(A) receptor. Nat Rev Neurosci. 2005;6(7):565–575. doi:10.1038/nrn1703
-
Berin E et al. Resistance training for hot flushes in postmenopausal women: A randomised controlled trial. Maturitas. 2019;126:55–60. doi:10.1016/j.maturitas.2019.05.005
-
Bianchi MT et al. Nocturnal Hot Flashes: Relationship to Objective Awakenings and Sleep Stage Transitions. J Clin Sleep Med. 2016;12(7):1003–1009. doi:10.5664/jcsm.5936
-
Bixler EO et al. Prevalence of Sleep-Disordered Breathing in Women: Effects of Gender. Am J Respir Crit Care Med. 2001;163(3):608–613. doi:10.1164/ajrccm.163.3.9911064
-
Yu J, Zhou Z, Cao X. Prevalence of poor sleep quality during menopause: a meta-analysis. Sleep and Breathing. 2024;28(6):2663–2674. doi:10.1007/s11325-024-03132-y · PMID:39145901
-
Caufriez A et al. Progesterone prevents sleep disturbances and modulates GH, TSH, melatonin secretion in postmenopausal women. J Clin Endocrinol Metab. 2011;96(4):E614–E623. PMID:21289261
-
Huang T, Lin BM, Redline S, Curhan GC, Hu FB, Tworoger SS. Type of Menopause, Age at Menopause, and Risk of Developing Obstructive Sleep Apnea in Postmenopausal Women. Am J Epidemiol. 2018;187(7):1370–1379.
-
Joffe H, White DP, Crawford SL et al. Adverse effects of induced hot flashes on objectively recorded and subjectively reported sleep: results of a gonadotropin-releasing hormone agonist experimental protocol. Menopause. 2013;20(9):905–914. doi:10.1097/GME.0b013e31828292d1 · PMID:23481119
-
Kravitz HM et al. Sleep disturbance during the menopausal transition in a multi-ethnic community sample of women. Sleep. 2008;31(7):979–990. PMID:18652093
-
Lampio L et al. Sleep during menopausal transition: a 10-year follow-up. Sleep. 2021;44(7):zsab008.
-
Lederman S et al. Fezolinetant for treatment of moderate-to-severe vasomotor symptoms associated with menopause (SKYLIGHT 1): a phase 3 randomised controlled study. Lancet. 2023;401(10382):1091–1102.
-
Marlatt KL et al. Body composition and cardiometabolic health across the menopause transition. Obesity. 2022;30(1):14–27. doi:10.1002/oby.23289
-
Nolan BJ et al. Efficacy of Micronized Progesterone for Sleep: A Systematic Review and Meta-analysis. J Clin Endocrinol Metab. 2021;106(4):e942–e950. PMID:33245776
-
Pinkerton JV, Simon JA, Joffe H et al. Elinzanetant for the Treatment of Vasomotor Symptoms Associated with Menopause: OASIS 1 and 2 Phase 3 Trials. JAMA. 2024;332(16):1343–1354. PMC11342219
-
Thurston RC et al. Trajectories of Sleep Over Midlife and Incident Cardiovascular Disease Events in the Study of Women’s Health Across the Nation. Circulation. 2024;149(7):545–555.
-
Wang Y, Liu H, Zhou B et al. Menopause and obstructive sleep apnea: revealing an independent mediating role of visceral fat beyond body mass index. BMC Endocr Disord. 2025;25:21. doi:10.1186/s12902-025-01850-2 · PMID:39863851
-
Zuraikat FM et al. Chronic Insufficient Sleep in Women Impairs Insulin Sensitivity Independent of Adiposity Changes: Results of a Randomized Trial. Diabetes Care. 2024;47(1):117–125. PMID:37955852
Why can't I sleep through the night anymore in perimenopause?
Three biological systems shift at the same time: progesterone (and its calming brain metabolite allopregnanolone) declines, the heat-regulation centre in the hypothalamus becomes unstable and triggers nocturnal hot flashes, and upper-airway muscle tone weakens. Each axis on its own can disrupt sleep continuity. In many women all three are at play.
What does progesterone have to do with my sleep?
Progesterone is converted in the brain into allopregnanolone, a compound that activates the same calming brake on neurons that benzodiazepines target, without the dependency profile. When progesterone falls in perimenopause, this endogenous deep-sleep switch falls with it. Oral micronised progesterone at bedtime has evidence for restoring this effect, but it requires a prescription.
Does the risk of sleep apnea rise during menopause?
Yes, substantially. Postmenopausal women carry roughly two to three times the risk of obstructive sleep apnea compared to premenopausal women. Oestrogen and progesterone help maintain upper-airway muscle tone. When that protection fades, nocturnal breathing pauses become more frequent. Women are still under-diagnosed because they snore more quietly and present with insomnia and fatigue rather than classic daytime sleepiness.
Which micronutrients can support sleep in perimenopause?
Magnesium bisglycinate or magnesium L-threonate (200 to 400 mg at bedtime), glycine (3 g) and L-theanine (200 mg) all show improvements in subjective sleep quality in trials. They do not replace diagnostics, but they can play a supporting role once your hormonal and metabolic foundation has been checked.
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.