Hormones
Does Perimenopause Change Your Gut? What the Research Shows and What You Can Do
9 June 2026 · By Dr. B.J. Huber · 13 min read
It often starts quietly. Your belly feels bloated in the evening, even though nothing about your diet has changed. Your gut becomes sluggish or unpredictable. Foods you have tolerated for years suddenly sit heavily. And at some point you start to wonder whether it is connected to your hormones.
I know this from my own experience. I had gut problems as a child along with an exhaustion that nobody could explain, and I now feel the first signs of the hormonal shift myself. That is exactly why I looked at the studies on this topic so closely.
What I found surprised me. On social media, the link between the gut and perimenopause is sold as established fact, almost always under one buzzword: the estrobolome. The research behind it is far more cautious. This article shows you what is genuinely proven, what is overstated, and above all, which levers you can pull yourself to bring some calm back to your gut.
- The hormonal shift begins quietly, earlier than most expect: as early as the mid-to-late 30s, ovarian reserve and progesterone decline step by step while the cycle still looks normal (Hale et al., 2007; Harlow et al., 2012).
- Around menopause the gut microbiome measurably shifts. The best-supported finding is a drop in the bacteria that produce the protective messenger butyrate, along with a decline in estrobolome function (Peters et al., 2022).
- Two popular claims do not hold up: a meta-analysis found neither significantly lower bacterial diversity nor a changed Firmicutes-Bacteroidetes ratio (Front Endocrinol, 2026).
- Whether the change comes from the hormones or from companion factors such as diet, abdominal fat, and age cannot yet be cleanly separated in humans. This is precisely what makes an individual approach worthwhile.
- Good to know: you do not have to wait for perfect hormones. With gentle adjustments to your diet, movement, and sleep, you have real influence over your gut health. The concrete path is further down.
When does the hormonal shift actually begin?
Many assume the menopausal years start with the first hot flushes or irregular cycles. The hormonal groundwork is well under way by then. In the so-called late reproductive stage, which often begins in the mid-to-late 30s, ovarian reserve (measured via anti-Mullerian hormone, AMH) drops noticeably, and progesterone in the second half of the cycle declines step by step. The cycle itself often still looks regular in this phase (Hale et al., 2007; Harlow et al., 2012).
This matters for the gut, because progesterone influences gut movement. Even in a normal cycle, many women report looser stools, bloating, and abdominal pain just before menstruation, when progesterone and oestrogen fall (Bernstein et al., 2014). When these hormonal swings become larger and more unpredictable from the mid-30s onward, it makes sense that some women notice digestive changes early.
One honest caveat: the large microbiome studies compare women before and after menopause, not women at 35. We know little about the gut flora in this very early phase. What we can say is that the hormonal shift starts earlier than most people think.
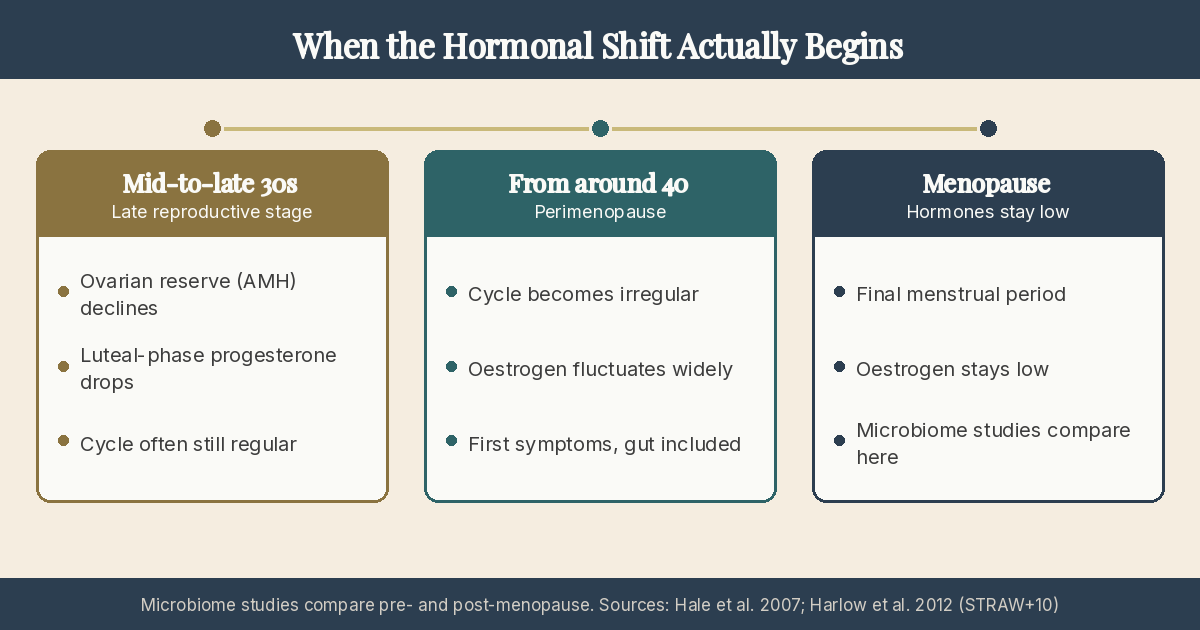 Fig. 1: The hormonal shift begins quietly, often as early as the mid-to-late 30s. The large gut microbiome studies, however, compare pre- and post-menopause (Hale et al., 2007; Harlow et al., 2012).
Fig. 1: The hormonal shift begins quietly, often as early as the mid-to-late 30s. The large gut microbiome studies, however, compare pre- and post-menopause (Hale et al., 2007; Harlow et al., 2012).
What measurably changes in the gut
This is where it gets concrete, and where I also need to set the evidence straight. There is exactly one adequately large human study on the gut microbiome around menopause: a study of more than 1,300 women in the US (Peters et al., 2022). All the other studies usually include only 20 to 90 women per group.
What holds up best across several studies:
- Fewer butyrate producers. Bacteria such as Roseburia, which make the short-chain fatty acid messenger butyrate (it nourishes the gut lining and acts anti-inflammatory), decline after menopause. This is the most reproducible single signal (Santos-Marcos et al., 2018; Peters et al., 2022).
- Less Akkermansia. This mucosa-friendly bacterium becomes rarer (Peters et al., 2022).
- The profile becomes more “male-like”. Before menopause, women’s gut flora differs more from that of same-age men than it does afterwards (Mayneris-Perxachs et al., 2020).
- Estrobolome function declines. The very bacterial activity that can reactivate excreted oestrogen decreases after menopause, rather than increasing (Peters et al., 2022). That does not fit neatly with the simple story I come to next.
This is a real but modest picture. The change exists, but it is smaller and more uncertain than most articles suggest.
The estrobolome: what holds up and what doesn’t
The term “estrobolome” comes from a 2011 concept paper and refers to the entirety of gut bacterial genes capable of processing oestrogen (Plottel and Blaser, 2011). Behind it sits real biochemistry: the liver breaks oestrogen down and sends it into the gut via bile. There, some bacteria can use the enzyme beta-glucuronidase to reactivate the oestrogen, so a portion returns to circulation.
So far, so well established. The leap that almost every site makes is the next one: that this estrobolome controls your oestrogen levels in perimenopause, and that you can fix it with the right supplement. The foundation for that is missing.
The key study on the mechanism was work done in a test tube and in mice. It showed that the enzymes can release oestrogen, but even a targeted inhibitor did not change the disease course in the mouse model (Ervin et al., 2019). A critical review from 2025 puts it plainly: the evidence is correlational, and direct control of circulating oestrogen by gut bacteria has not been observed in humans (Larnder et al., 2025). A longitudinal study following the same women through perimenopause, measuring gut flora and hormones in parallel, does not yet exist.
In short: the mechanism is plausible and interesting. As an explanation for your symptoms, or as the rationale for a particular supplement, it is not proven.
What many sites get wrong
Two claims appear in almost every text, and neither survives close scrutiny.
The first: “Bacterial diversity drops at menopause.” The second: “The Firmicutes-Bacteroidetes ratio rises.” Both sound well grounded. A 2026 meta-analysis that pooled several studies, however, found neither a significant difference in diversity nor in the Firmicutes-Bacteroidetes ratio (Front Endocrinol, 2026). An earlier study even found the ratio the other way around, higher in the younger women (Santos-Marcos et al., 2018).
The often-cited drop in Lactobacillus also needs context: it is well documented, but in the vaginal flora, not the gut. These two things are constantly mixed up.
Why does this matter for you? Because recommendations built on these shaky claims often miss the mark. Anyone promising a number about bacterial diversity that does not even show up reliably is selling a certainty that does not exist.
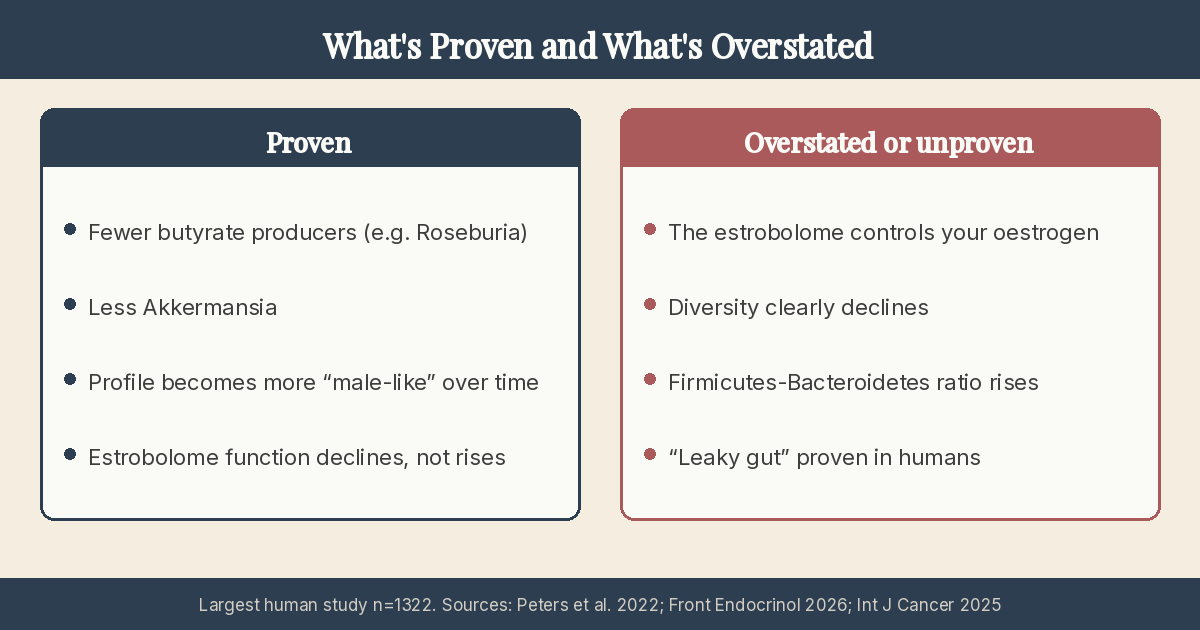 Fig. 2: What human studies actually show and what is claimed beyond that. The largest study included 1,322 women (Peters et al., 2022; Front Endocrinol, 2026; Int J Cancer, 2025).
Fig. 2: What human studies actually show and what is claimed beyond that. The largest study included 1,322 women (Peters et al., 2022; Front Endocrinol, 2026; Int J Cancer, 2025).
Is it the hormones, or diet, fat and age?
This is the most interesting question for me, and the honest answer is: it cannot yet be separated. Many things change at the same time around menopause. Oestrogen falls, age rises, abdominal fat often increases, diet shifts, movement and sleep decrease. Each of these factors affects the gut flora on its own.
One example makes this tangible: in one study, the differences between the women largely disappeared as soon as you looked only at the participants with obesity. One explanation is that fat tissue itself produces oestrogen (Mayneris-Perxachs et al., 2020). In other words, a good part of what is sold as a “menopause effect” could in truth be an effect of body fat, diet, or age.
The strongest pointer to a direct hormonal effect comes from animal studies: removing mice’s ovaries changes their gut flora, and giving oestrogen reverses it (Kaliannan et al., 2018). That is clean causal design, but it is a mouse and a surgical procedure, not the gradual human perimenopause. A controlled study of hormone therapy and gut flora in naturally menopausal women is still missing.
For you this means something freeing: if the cause is multi-layered, so are the levers. You have more influence than it feels like. Diet, movement, sleep, and weight are factors you can steer, and they probably act exactly where part of the change comes from. How to put this into practice is further down, in the section “What you can do for your gut now”.
Which symptoms actually become more common
The same honest lens is worth applying to symptoms.
The cyclical link is well established: when hormones fall, many women respond with bloating, abdominal pain, and altered bowel habits (Bernstein et al., 2014). This is the strongest evidence that sex hormones really do influence the gut.
For menopause specifically, the picture is thinner. There is a signal that women with irritable bowel syndrome have more severe symptoms after menopause than before, although from a small cross-sectional study in which age and menopause overlap (Lenhart et al., 2020). The circulating figure that three quarters of menopausal women suffer from bloating comes from an unpublished commercial survey and is not reliable as a prevalence.
You will often be warned that perimenopause inevitably leads to histamine intolerance or a leaky gut (a permeable gut barrier). Both ideas sound plausible, but neither is solidly proven in women in this phase. Before you invest in expensive tests or cut out healthy foods, it pays to start with the basics. The detailed evidence on both is in the FAQ at the end.
What you can do for your gut now
None of this leads to a dramatic programme, but to a calm, well-tolerated path. In perimenopause especially, aggressive standard tips can backfire. Suddenly eating 30 different plants a week, large amounts of fermented food, or high doses of sulphur-rich vegetables can irritate a sensitive gut in this phase. More on this in my article on gentle gut tips in perimenopause.
The order matters here: the oestrogen-gut loop only works with what the liver has broken down and delivered through the bile. So it pays to support the body as a whole rather than only tinkering with the gut.
Well-tolerated plant foods, at your own pace. The very butyrate producers that tend to decline live on fermentable plant fibre. What matters is tolerance: well-cooked, gently prepared vegetables are usually easier to handle than raw or strongly gas-forming amounts. Build up in small steps toward what suits you.
Eat enough protein. In the phase of life when muscle is harder to maintain, enough protein supports not only your muscles but also satiety and weight, and thereby indirectly one of the likely co-drivers of the gut change.
Treat movement as gut care. Strength training and moderate endurance work in different ways: strength helps maintain muscle and improve insulin sensitivity, while endurance stimulates gut movement and lowers stress, which acts on the gut through the gut-brain axis.
Take sleep and stress seriously. Both affect the gut-brain axis directly. When sleep suffers in perimenopause, the gut often suffers with it. How these systems connect is described in my article on brain fog, exhaustion, and the gut.
Reduce alcohol. Alcohol burdens the liver, which sits at the start of the oestrogen-gut loop, and irritates the gut lining.
Observe rather than restrict. Instead of cutting foods pre-emptively, a simple symptom diary over two to three weeks is worthwhile. That way you recognise what genuinely causes you problems and avoid needless restrictions.
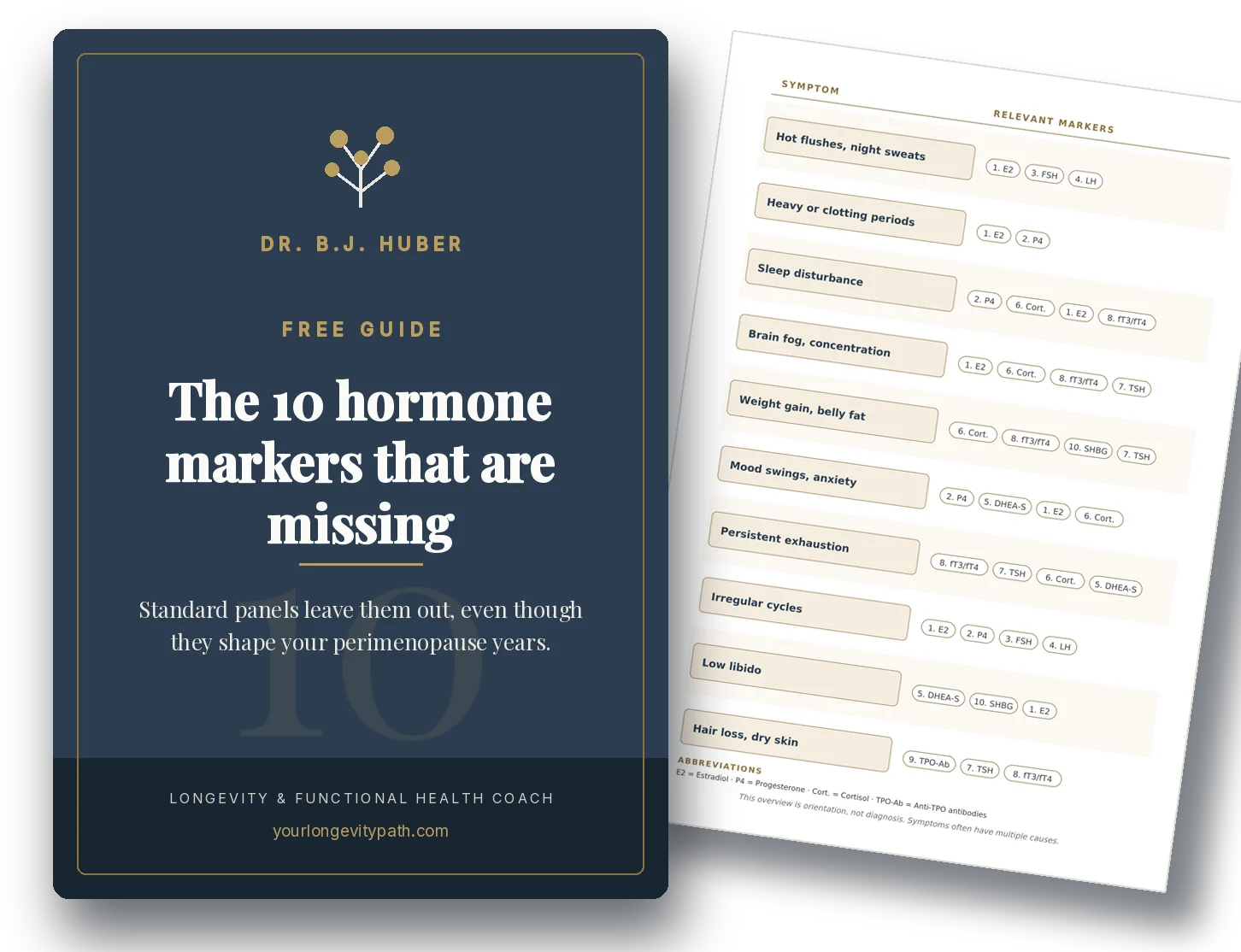
If you want to understand the hormonal background of your symptoms better, I have summarised the most important lab values in a guide to hormone markers.
Why there’s no one-size-fits-all
If you take one thing from this article, let it be this: the change in the gut is real, but it is individual. Research cannot trace it back to a single trigger, and that is exactly why no programme fits everyone. What helps one woman can leave another even more bloated.
This is an honest description of where the science stands. And it is the reason I work with you in coaching to identify which factors are interacting in your case and which levers make the biggest difference for you, rather than working with blanket prescriptions.
Birgit
If you would like to find out which levers make the most difference for you, my coaching for perimenopause offers the right framework, or you can start with a free initial consultation.
Scientific references
- Plottel CS, Blaser MJ. Microbiome and Malignancy. Cell Host Microbe. 2011;10(4):324–335. doi:10.1016/j.chom.2011.10.003 · PMID:22018233
- Ervin SM, Li H, Lim L, et al. Gut microbial β-glucuronidases reactivate estrogens as components of the estrobolome. J Biol Chem. 2019;294(49):18586–18599. doi:10.1074/jbc.RA119.010950 · PMID:31636122
- Larnder AH, Manges AR, Murphy RA. The estrobolome: Estrogen-metabolizing pathways of the gut microbiome and their relation to breast cancer. Int J Cancer. 2025. doi:10.1002/ijc.35427 · PMC12178105
- Peters BA, Lin J, Qi Q, et al. Menopause Is Associated with an Altered Gut Microbiome and Estrobolome, with Implications for Adverse Cardiometabolic Risk. mSystems. 2022;7(3):e00273-22. doi:10.1128/msystems.00273-22
- Santos-Marcos JA, Rangel-Zuñiga OA, Jimenez-Lucena R, et al. Influence of gender and menopausal status on gut microbiota. Maturitas. 2018;116:43–53. doi:10.1016/j.maturitas.2018.07.008 · PMID:30244778
- Mayneris-Perxachs J, et al. Gut microbiota steroid sexual dimorphism and its impact on gonadal steroids. Microbiome. 2020;8(1):136. doi:10.1186/s40168-020-00913-x
- The impact of estrogen status on the gut microbiome: a systematic review and meta-analysis. Front Endocrinol. 2026;17:1780806. doi:10.3389/fendo.2026.1780806
- Kaliannan K, Robertson RC, Murphy K, et al. Estrogen-mediated gut microbiome alterations influence sexual dimorphism in metabolic syndrome in mice. Microbiome. 2018;6(1):205. doi:10.1186/s40168-018-0587-0
- Lenhart A, Naliboff B, Shih W, et al. Postmenopausal women with irritable bowel syndrome have more severe symptoms than premenopausal women. Neurogastroenterol Motil. 2020;32(10):e13913. doi:10.1111/nmo.13913
- Bernstein MT, Graff LA, Avery L, et al. Gastrointestinal symptoms before and during menses in healthy women. BMC Womens Health. 2014;14:14. doi:10.1186/1472-6874-14-14
- Maintz L, Novak N. Histamine and histamine intolerance. Am J Clin Nutr. 2007;85(5):1185–1196. doi:10.1093/ajcn/85.5.1185
- Hamada Y, Shinohara Y, Yano M, et al. Effect of the menstrual cycle on serum diamine oxidase levels in healthy women. Clin Biochem. 2013;46(1–2):99–102. doi:10.1016/j.clinbiochem.2012.10.013
- Braniste V, Leveque M, Buisson-Brenac C, et al. Oestradiol decreases colonic permeability through oestrogen receptor β-mediated up-regulation of occludin and junctional adhesion molecule-A in epithelial cells. J Physiol. 2009;587(13):3317–3328. doi:10.1113/jphysiol.2009.169300
- Zhou Z, Zhang L, Ding M, et al. Estrogen decreases tight junction protein ZO-1 expression in human primary gut tissues. Clin Immunol. 2017;183:174–180. doi:10.1016/j.clim.2017.08.019 · PMID:28867253
- Collins FL, Rios-Arce ND, Schepper JD, et al. Ovariectomy-induced estrogen deficiency alters gut permeability and tight junction gene expression. 2017. PMC5430124
- Harlow SD, Gass M, Hall JE, et al. Executive summary of the Stages of Reproductive Aging Workshop +10. J Clin Endocrinol Metab. 2012;97(4):1159–1168. doi:10.1210/jc.2011-3362
- Hale GE, Zhao X, Hughes CL, et al. Endocrine features of menstrual cycles in middle and late reproductive age and the menopausal transition classified according to the STRAW staging system. J Clin Endocrinol Metab. 2007;92(8):3060–3067. doi:10.1210/jc.2007-0066 · PMID:17550960
Does the gut really change during perimenopause?
Yes, but the evidence is thinner than many sites claim. Human studies show the composition of the gut microbiome shifts around menopause, above all fewer bacteria that produce the protective messenger butyrate. Most studies, however, are small and compare different women at one point in time rather than the same woman over the years.
Does the hormonal shift begin as early as the mid-30s?
The quiet phase does. In the late reproductive stage, often from the mid-to-late 30s, ovarian reserve (AMH) and luteal-phase progesterone decline step by step while the cycle still looks normal (Hale et al., 2007; Harlow et al., 2012). This is why some women notice digestive changes long before classic perimenopause begins.
Is it true that the estrobolome controls my oestrogen?
The mechanism exists: some gut bacteria can reactivate excreted oestrogen. But that this estrobolome measurably controls oestrogen levels in humans is not proven. The key study was cell and mouse work (Ervin et al., 2019), and a critical review notes that direct causation has not been observed in humans (Larnder et al., 2025).
What can I do for my gut during perimenopause?
Go gently rather than with a shock programme. Eat well-tolerated plant foods at your own pace, get enough protein, keep movement, sleep, and stress in view, and reduce alcohol. Aggressive standard tips such as suddenly eating 30 plants a week or large amounts of fermented food can make symptoms worse in this phase.
Will perimenopause give me histamine intolerance or a leaky gut?
Both are seen as plausible mechanisms but are not solidly proven in women during perimenopause. For histamine intolerance, the only human study on the cycle even found the breakdown enzyme DAO higher in the second half of the cycle (Maintz and Novak, 2007; Hamada et al., 2013); a defined perimenopausal histamine intolerance does not exist as a diagnosis. For leaky gut, mostly animal studies support the idea, direct measurements in menopausal women are missing, and the animal data even contradict each other on the direction (Braniste et al., 2009; Zhou et al., 2017; Collins et al., 2017).
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.