Hormones
Creatine in Perimenopause: What It Really Does, Beyond Muscle
18 June 2026 · By Dr. B.J. Huber · 10 min read
When I think of creatine, the first image that comes up is the one most people have: muscle building, the powder in the trainer and bodybuilder scene, young men at the gym. That is exactly why creatine is so underrated. Because muscle is almost the least interesting part of the story.
I am a natural scientist, and when I read studies in the evening, what interests me about a substance is always the mechanism, not the promise on the tub. Creatine is exactly where I got stuck: what is sold as a muscle powder is in truth a story about cellular energy. And it became genuinely fascinating to me when I felt the first signs of the hormonal shift in my own body.
This article lays bare the core mechanisms, separates evidence from claim, and shows you why creatine can make sense precisely in this phase of life, without me selling you a hormone miracle.
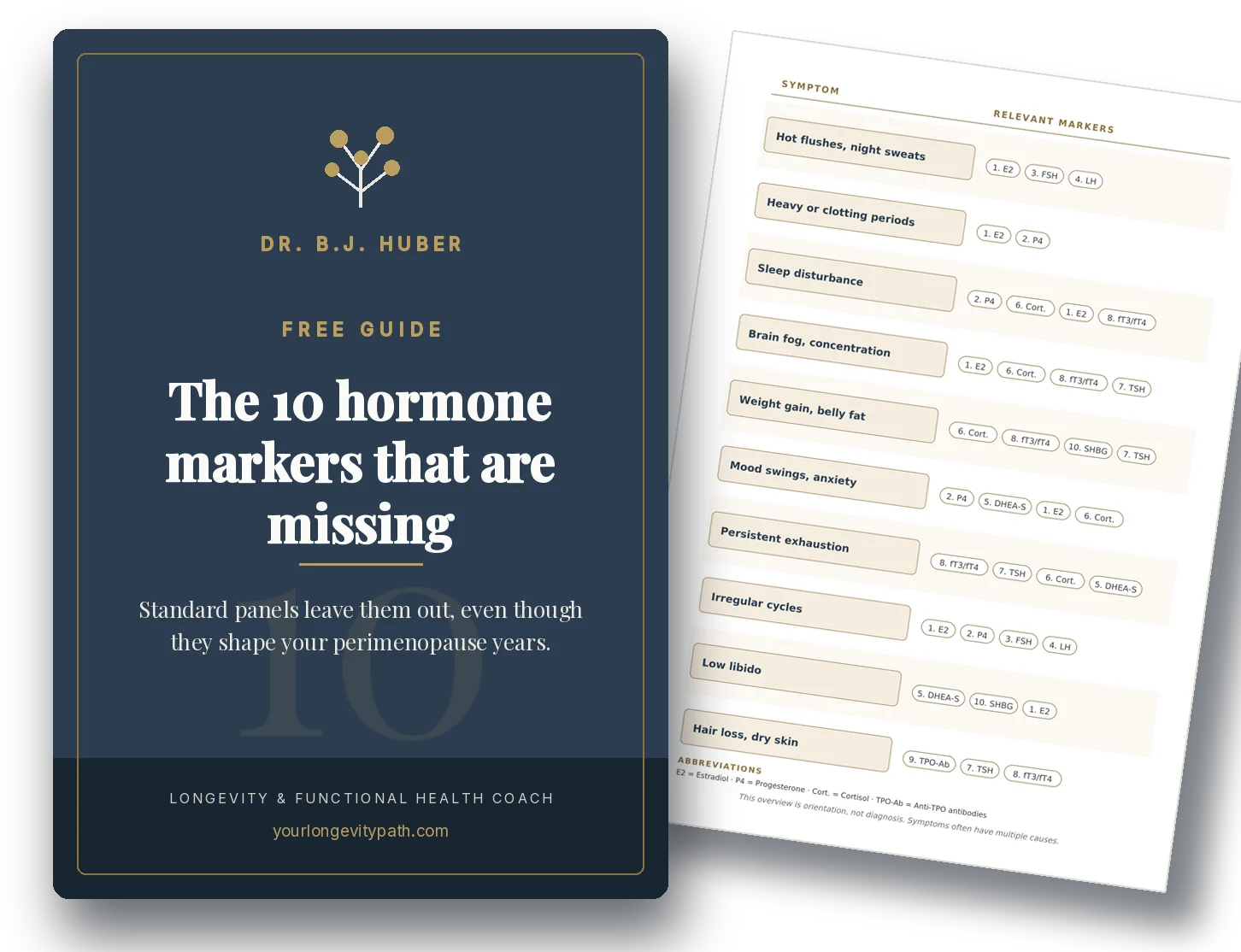
- Cellular energy: Creatine stores fast energy and releases it instantly under load, not only in muscle but also in the brain.
- Methylation: Your body’s own creatine synthesis uses around 40 per cent of all methyl groups (Brosnan and Brosnan, 2011). Supplementing creatine spares them.
- Hormones, soberly considered: Creatine does not directly improve any hormone production. The link runs the other way, oestrogen regulates the creatine system (Smith-Ryan et al., 2021).
- Women’s stores: 70 to 80 per cent lower than men’s. When oestrogen fluctuates and falls, that is the reason to top up the stores.
- How to take it: Creatine monohydrate, daily, very well studied and safe. Not a hormone replacement, but a support for cellular energy.
The core element: cellular energy
Everything creatine does hangs on a single system. Every cell needs energy in the form of ATP. Under a sudden load, ongoing ATP production cannot keep up fast enough. A thought, a muscle movement, a heartbeat: that is when the phosphocreatine system steps in. It donates a phosphate group very quickly and makes ATP available exactly where it is missing. Creatine is therefore an energy store for short peaks.
That is why creatine sits everywhere a lot of energy is needed, not only in muscle but also in the brain and the heart. In muscle it is simply most noticeable.
One important clarification, especially against the “mitochondria booster” marketing: for a long time creatine was described as an energy transporter that shuttles energy across the cell. Newer calculations show that this transport accounts for only a small part and that the storage function clearly dominates (Hettling and van Beek, 2011). So creatine is not a miracle cure for the mitochondria, but a reliable energy store. And that is already a lot.
Methylation: why creatine and oestrogen are connected
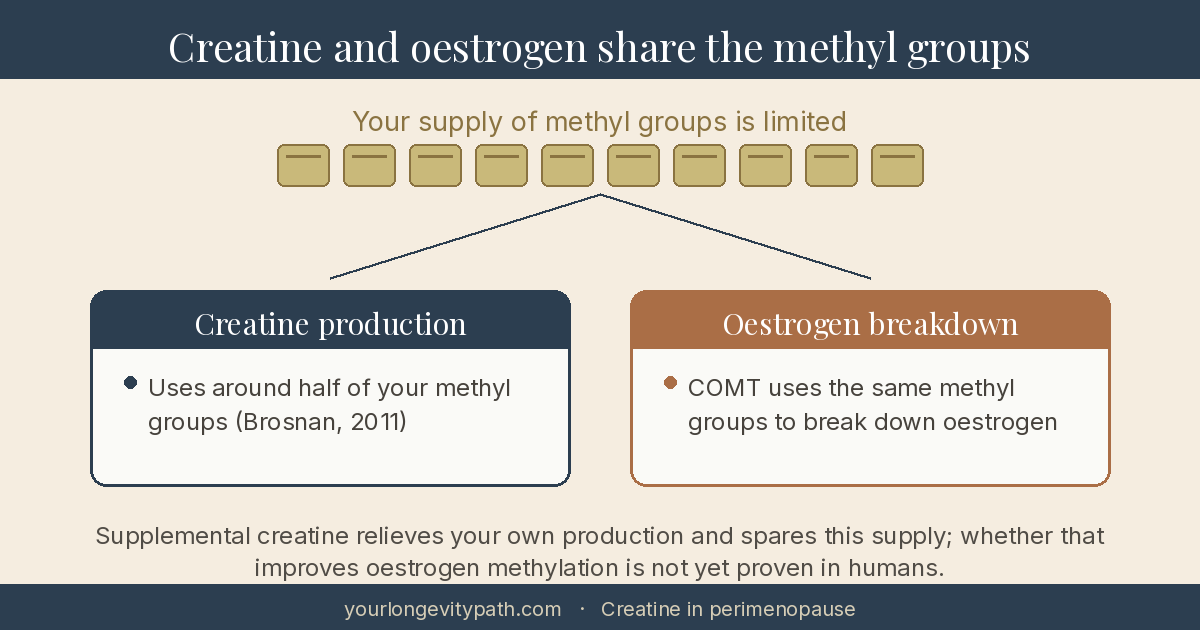
This part I understood late myself. Your body also makes creatine on its own, in two steps. The final step happens in the liver and uses up one methyl group. That sounds like little, but it is a lot: creatine production is the single largest consumer of methyl groups in the body, using around 40 per cent of them (Brosnan and Brosnan, 2011).
Methyl groups are scarce. The body also needs them for DNA regulation, for messenger substances and, particularly interesting for perimenopause, for the breakdown of oestrogen via the enzyme COMT. When you supplement creatine, the body has to make less of its own and spares exactly these methyl groups. The obvious hypothesis: this spared capacity is then available for other tasks, in theory also for oestrogen detoxification.
But here I have to put on the brakes, otherwise a good hypothesis turns into a false promise. In a controlled trial in adults, creatine did lower the precursor guanidinoacetate, but on average it did not lower homocysteine, the marker of methylation. It dropped only in a subgroup that took creatine together with folic acid (Peters et al., 2015). So the mechanism is coherent and plausible, but a direct easing of methylation in humans is not established. Fascinating, yes. Proven, no. If you want to know which values such as homocysteine even make sense in this phase, you will find that in my article on blood tests in perimenopause.
Energy for the brain
Because the brain consumes an enormous amount of energy and has its own creatine stores, it is the second large field of application. Here the research shows the most interesting effects, especially under strain.
In one study, even a single high dose of creatine improved mental performance after a sleepless night and prevented the brain’s energy reserves from collapsing (Gordji-Nejad et al., 2024). A review found that creatine improves above all reasoning and short-term memory, most clearly where the stores are naturally low, for example in older people and in vegetarians (Avgerinos et al., 2018).
That is relevant because many women in perimenopause complain about exactly these symptoms: brain fog, worse concentration, word-finding trouble, often together with poorer sleep. This mix of exhaustion and a head running in fog is something I know from my own experience, and it was one of the reasons I looked so closely at the cell’s energy system. How this exhaustion fits together I describe in the article on exhaustion and burnout in perimenopause.
For a long time the data specifically on women was thin. That is changing right now: in 2025 the first controlled studies directly in peri- and postmenopausal women appeared. In one of them (CONCRET-MENOPA), creatine over eight weeks improved reaction time and softened mood swings, and the creatine content in the frontal brain rose measurably (J Am Nutr Assoc, 2025). A further study in menopausal women saw effects on cognition, strength and sleep (PMC12291186, 2025). The studies are real, but still small and short. That does not yet make creatine a proven remedy against brain fog, but an increasingly well-founded candidate.
The hormone question, turned around
Now to the question that intrigues me most about this topic, partly because I now read marketing promises around women’s hormones with a certain scepticism since I am in this phase myself: does creatine directly help to improve hormone production? The sober answer is no. The interesting thing is the other direction.
First, the myth.
The myth: Creatine raises testosterone.
What the data show: The claim rests on a single, never-replicated crossover study in 20 young rugby players. There, after a high-dose initial week, DHT, a breakdown product of testosterone, rose by 56 per cent but stayed within the clinical normal range, and testosterone itself did not change (van der Merwe et al., 2009). In the majority of the remaining studies, testosterone does not move at all (Antonio et al., 2021). A single, unconfirmed paper carries no statement about hormonal effect. You will find more on this in my article on testosterone for women in perimenopause.
The genuinely important insight is the reverse direction: it is not creatine that steers the hormones, but the hormones that steer the creatine system. Oestrogen demonstrably regulates the rate-limiting synthesis step (the enzyme AGAT) and the activity of creatine kinase, and creatine kinase fluctuates across the cycle along with oestrogen (Smith-Ryan et al., 2021). Women already have creatine stores 70 to 80 per cent lower than men.
From this follows the logic of this article: because oestrogen co-steers the creatine system, your own production runs less well as soon as oestrogen fluctuates and falls in perimenopause. That is why it is worth topping up the stores. Creatine fills them, but it does not change your hormones.
What this means in practice: dose and safety
If you would like to try creatine, it is straightforward:
- Form: Creatine monohydrate, the best-studied and cheapest variant. More expensive forms bring no proven added value.
- Taken daily and long term, independent of training.
- Clarify with your physician in case of kidney disease, during pregnancy or while breastfeeding.
Creatine monohydrate is one of the most thoroughly studied and safest supplements there is (Antonio et al., 2021).
Creatine unfolds its greatest benefit not on its own but together with strength training, especially after menopause for muscle and bone. That connects directly to a topic from my article on the weight-loss injections in perimenopause: anyone who loses weight or ages also loses muscle, and it is exactly this muscle preservation that creatine and strength training support together. How closely muscle, protein and insulin are linked I go into in the article on insulin resistance in perimenopause.
Why it fits your phase
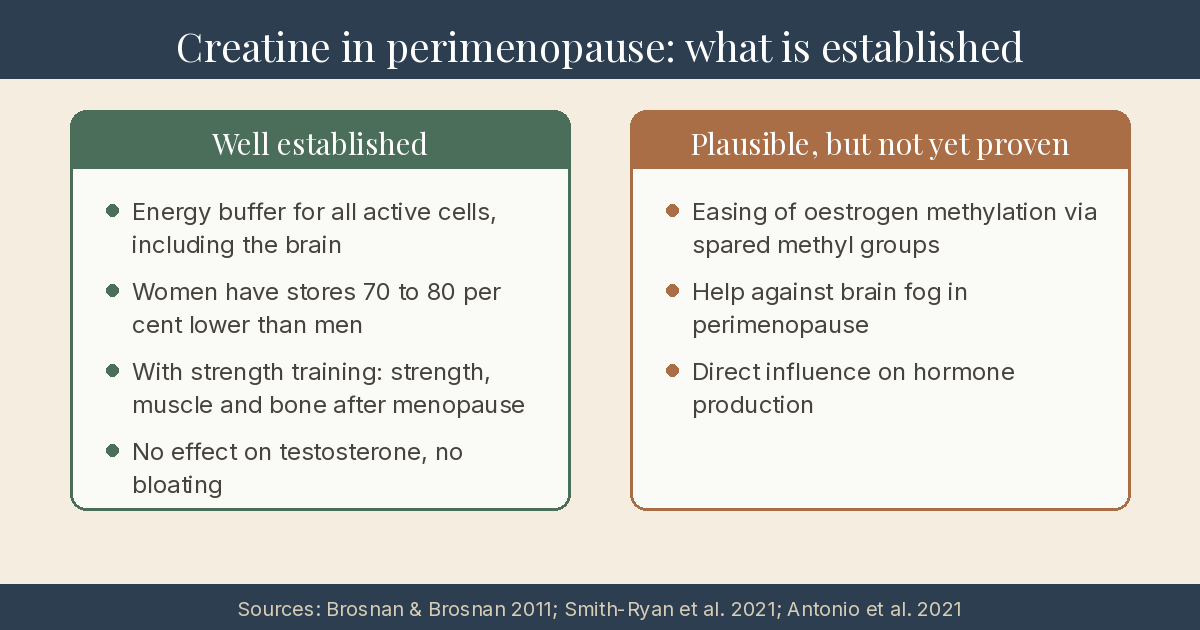
Let us sum up. Creatine is not a hormone agent and not a miracle cure for the mitochondria. It is a well-established energy store for the cell, a plausible reliever of methylation, and a promising supporter for the brain that is visible in the first studies in women but not yet established. It fits perimenopause because of the hormonal situation: a system that is co-steered by oestrogen and is already more sparsely equipped in women benefits from being topped up when oestrogen fluctuates and falls.
That is no sensation, but something better: a mechanistically grounded support where you know exactly what it can do and what it cannot.
That is exactly how I work in coaching too: looking at which building blocks fit together sensibly in your case, instead of selling single agents as miracle cures.
Birgit
If you would like to find out which levers make the most difference for you, my coaching for perimenopause offers the right framework, or you can start with a free initial consultation.
Scientific Sources
- Brosnan JT, Brosnan ME. The metabolic burden of creatine synthesis. Amino Acids. 2011;40(5):1325–1331. doi:10.1007/s00726-011-0853-y · PMID:21387089
- Peters BA, Hall MN, Liu X, et al. Low-dose creatine supplementation lowers plasma guanidinoacetate, but not plasma homocysteine, in a double-blind, randomized, placebo-controlled trial. J Nutr. 2015;145(10):2245–2252. PMID:26311810
- Hettling H, van Beek JHGM. Analyzing the functional properties of the creatine kinase system with multiscale sloppy modeling. PLoS Comput Biol. 2011;7(8):e1002130. doi:10.1371/journal.pcbi.1002130
- Smith-Ryan AE, Cabre HE, Eckerson JM, Candow DG. Creatine supplementation in women’s health: a lifespan perspective. Nutrients. 2021;13(3):877. doi:10.3390/nu13030877 · PMC7998865
- van der Merwe J, Brooks N, Myburgh KH. Three weeks of creatine monohydrate supplementation affects dihydrotestosterone to testosterone ratio in college-aged rugby players. Clin J Sport Med. 2009;19(5):399–404. doi:10.1097/JSM.0b013e3181b8b52f · PMID:19741313
- Antonio J, Candow DG, Forbes SC, et al. Common questions and misconceptions about creatine supplementation: what does the scientific evidence really show? J Int Soc Sports Nutr. 2021;18(1):13. doi:10.1186/s12970-021-00412-w · PMC7871530
- Gordji-Nejad A, Matusch A, Kleedörfer S, et al. Single dose creatine improves cognitive performance and induces changes in cerebral high energy phosphates during sleep deprivation. Sci Rep. 2024;14:4937. doi:10.1038/s41598-024-54249-9 · PMC10902318
- Avgerinos KI, Spyrou N, Bougioukas KI, Kapogiannis D. Effects of creatine supplementation on cognitive function of healthy individuals: a systematic review of randomized controlled trials. Exp Gerontol. 2018;108:166–173. doi:10.1016/j.exger.2018.04.013
- The effects of 8-week creatine hydrochloride and creatine ethyl ester supplementation on cognition, clinical outcomes, and brain creatine levels in perimenopausal and menopausal women (CONCRET-MENOPA): a randomized controlled trial. J Am Nutr Assoc. 2025;45(3). doi:10.1080/27697061.2025.2551184
- Impact of creatine supplementation on menopausal women’s body composition, cognition, estrogen, strength, and sleep. 2025. PMC12291186
Does creatine only act on muscle?
No, muscle is almost the least interesting part. The core of creatine is cellular energy. Through the phosphocreatine system it stores fast energy and releases it on demand, in every active tissue, including the brain and the heart. Muscle is simply the most visible example.
Does creatine raise testosterone or hormone production?
No. Creatine does not directly improve any hormone production. The widespread testosterone myth rests on a single, never-replicated crossover study in 20 rugby players. There, DHT rose by 56 per cent but stayed within the normal range, and testosterone itself did not change (van der Merwe et al., 2009). The relationship runs the other way: oestrogen regulates the creatine system, not creatine the hormones.
Why is creatine particularly interesting in perimenopause?
Women naturally have creatine stores 70 to 80 per cent lower than men, and oestrogen regulates key steps of creatine metabolism (Smith-Ryan et al., 2021). When oestrogen fluctuates and falls, your own production runs less well. That is why it is worth topping up the stores. But creatine does not change your hormones.
What does creatine have to do with methylation and the liver?
Your body's own creatine synthesis completes in the liver and is the single largest consumer of methyl groups in the body, using around 40 per cent of them (Brosnan and Brosnan, 2011). Supplementing creatine spares these methyl groups. Whether that also eases oestrogen detoxification is a coherent hypothesis, but not proven in humans (Peters et al., 2015).
How do you take creatine and is it safe?
The best-studied and cheapest form is creatine monohydrate, taken daily and long term. It is one of the most thoroughly studied and safest supplements there is (Antonio et al., 2021). With kidney disease, in pregnancy or while breastfeeding, taking it should be discussed with your physician.
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.