Longevity
Do we age faster in perimenopause? Why your mitochondria hold the answer
15 May 2026 · By Dr. B.J. Huber · 12 min read
You might remember what it felt like at 35 or 38: a hard workout, a short night, a stressful day, and the next morning you were back in the game. Today, after the same load, you need two days, sometimes three. You go to bed at ten and still wake up unrested at seven. By mid-afternoon your energy drops into a hole that a coffee no longer reliably pulls you out of.
It feels like a character flaw or a lack of discipline. It is neither. A central shift is unfolding in your cells that begins long before you classically feel like you are “in the change”. Oestrogen has been a direct protective factor for your mitochondria, the powerhouses of your cells, for decades. As it declines, their efficiency declines too. Fatigue, exercise intolerance and slow recovery are then not in your head; they are measurable.
This article walks through the research on what happens in your cells during perimenopause, why biological ageing accelerates in this window, and which interventions have the strongest evidence for restoring your cellular energy.
- Oestrogen regulates mitochondrial biogenesis and protects mitochondria against oxidative stress. When it falls, cellular energy production drops measurably.
- Levine and colleagues (2016) analysed over 3,000 women and showed that menopause accelerates biological ageing in blood. Earlier menopause and a longer time since the final period both predict higher age acceleration.
- The strongest levers are strength training with short intervals, sleep quality, protein distribution, sauna and a solid micronutrient base. Mitochondria remain trainable at any age.
What do mitochondria have to do with perimenopause?
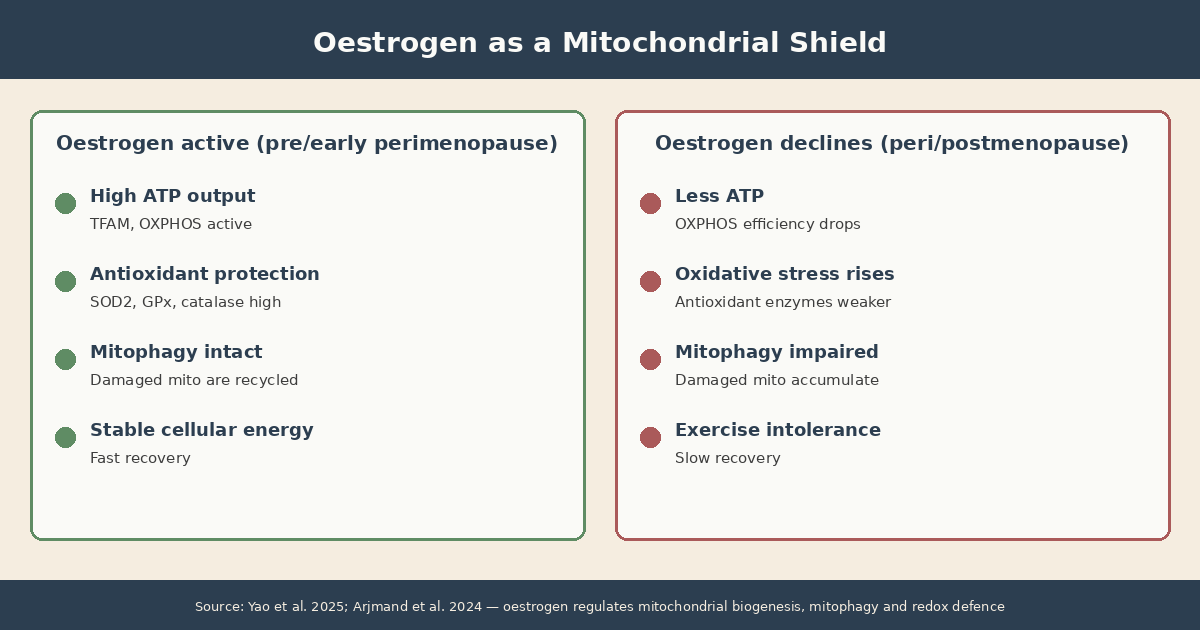
Mitochondria produce more than 90 per cent of your cellular energy in the form of ATP. Oestrogen directly regulates how many mitochondria your cells build, how well they work and how effectively they defend themselves against oxidative stress. When oestrogen falls, that protection weakens.
A 2025 review describes the molecular mechanism in detail. Oestradiol binds to oestrogen receptors located inside the mitochondria themselves and switches on two protective systems. The first makes sure your cells keep building enough clean, new mitochondria (via a central read-switch for mitochondrial DNA, referred to in the literature as TFAM). The second is the cell’s own fire brigade against oxidative stress, the harmful by-products of metabolism (enzymes such as SOD2, GPx and catalase). Oestrogen also fuels mitophagy, the clean-up process that recycles damaged mitochondria (Yu et al., 2025).
When oestrogen becomes erratic in perimenopause and ultimately declines, this finely tuned system destabilises. Mitochondrial efficiency drops, oxidative stress rises and damaged mitochondria are cleared more slowly. The result: less ATP at the same workload, longer recovery times and more low-grade inflammation.
This explains a real share of what feels subjectively like rapid ageing. Cells produce less energy per oxygen molecule while running under more oxidative stress. The effect hits every energy-hungry tissue at once: brain, heart, skeletal muscle, liver and ovaries.
Does menopause really accelerate biological ageing?
Yes, and the evidence is solid. A study by Levine and colleagues (2016) analysed data from over 3,000 women across four large cohorts and found that menopause accelerates epigenetic ageing in blood. Earlier menopause and a longer time since the final period both correlate with higher biological age acceleration.
The study used the Horvath epigenetic clock, a biomarker that estimates biological age from DNA methylation patterns. Women who had undergone bilateral oophorectomy (surgical menopause) showed measurably accelerated epigenetic ageing compared with women whose ovaries remained intact. A Mendelian randomisation analysis using genetic variants linked to age at menopause supported the relationship — though the effect was observed only in blood, not in buccal epithelium or saliva, so causality is suggested but not definitively established (Levine et al., 2016).
Clinically, this means menopause is not a neutral milestone. It is a phase during which biological ageing processes are accelerated. That is information, not a verdict. The same research field also shows that the levers known to slow this acceleration (exercise, sleep, micronutrients, stress regulation) are particularly effective during midlife.
Why does the fatigue feel like it is everywhere?
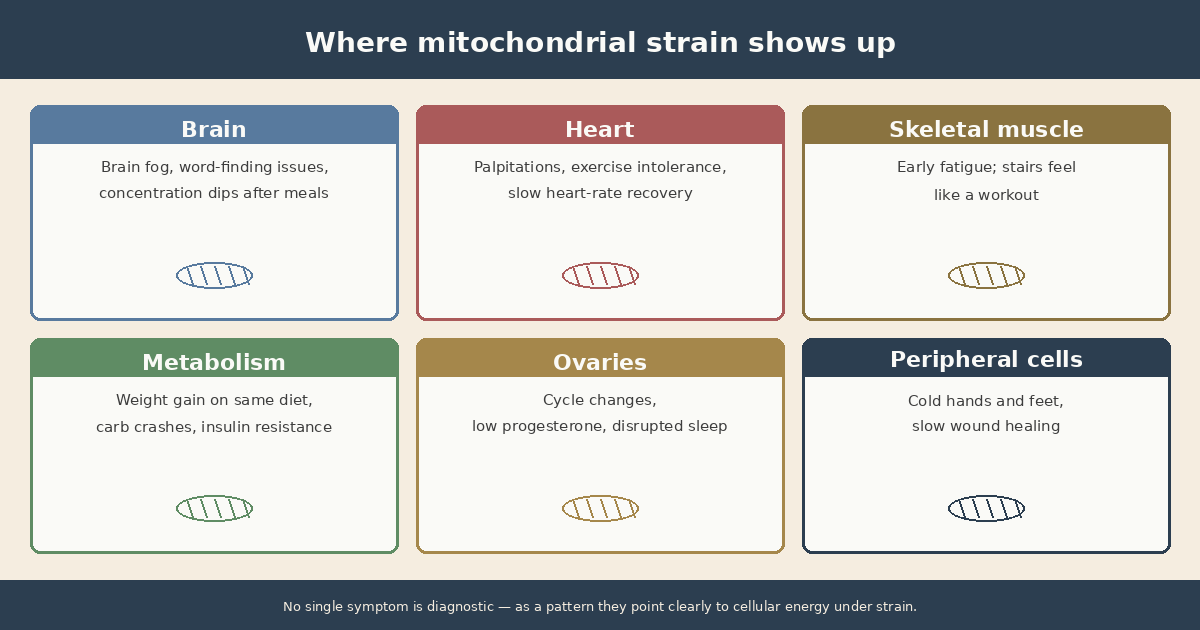
Because mitochondria sit in every tissue that consumes a lot of energy. When their efficiency drops, the effect is not localised. You feel it in your head, your heart, your muscles and your hormonal control system at the same time.
A cardiac muscle cell holds 5,000 to 6,000 mitochondria. A skeletal muscle cell holds 200 to 1,000. Brain neurons hold hundreds. The brain uses around 20 per cent of total metabolic energy while making up only 2 per cent of body weight. When mitochondrial function drops, the effect hits everywhere at once.
Lisa Mosconi’s group at Weill Cornell Medicine has studied this in detail in the female brain. Using FDG-PET imaging, they showed that perimenopausal and postmenopausal women exhibit hypometabolism in the same brain regions affected during the early phase of Alzheimer’s disease. The researchers describe this as a “bioenergetic crisis” in the female brain that begins in midlife (Mosconi et al., 2017). In parallel, Roberta Brinton’s group documented in a rodent study that mitochondrial respiration in the female brain declines during the perimenopausal transition and that synaptic plasticity measurably shifts (Yin et al., 2015).
This is not a forecast of disease. It does, however, explain why cognitive symptoms such as brain fog, word-finding difficulties and concentration problems are so common in perimenopause, and why the same levers that protect mitochondria also protect the brain. For a deeper dive into how brain fog emerges in this transition, see our article on perimenopause and gut-brain interaction.
What happens to NAD+ and SIRT1 after 40?
NAD+ (nicotinamide adenine dinucleotide) is the central coenzyme of your mitochondria. It drives ATP production and acts as the substrate for sirtuins, a family of enzymes considered cellular longevity sensors. NAD+ declines with age, and in perimenopause the loss of oestrogenic protection compounds that decline.
Sirtuins, particularly SIRT1 and SIRT3, regulate mitochondrial biogenesis, mitophagy and antioxidant defence. To function, they need NAD+. When NAD+ drops, sirtuin activity drops with it, and the cell shifts into a less protected mode.
Clinical trials of NAD+ precursors (NMN, NR) paint a consistent picture: both reliably raise NAD+ levels in blood. A randomised controlled trial in postmenopausal women with prediabetes showed that 250 mg of NMN daily significantly improved muscle insulin sensitivity (Yoshino et al., 2021). A 12-week trial in older adults improved sleep quality and gait speed (Morifuji et al., 2024). Other endpoints (cognition, fatigue, cardiovascular function) show mixed results so far.
My takeaway from the current evidence: NMN and NR are interesting, but not an automatic game-changer. The NAD+ axis also responds well to lifestyle: regular exercise, sufficient sleep, moderate calorie intake and occasional fasting all raise NAD+ measurably, without any supplement. Anyone considering supplementation should do so with medical guidance, not as a substitute for the non-pharmacological levers.
Which symptoms point to mitochondrial strain in perimenopause?
Mitochondrial dysfunction rarely shows up as one isolated symptom. It shows up as a pattern of exercise intolerance, slow recovery and energy crashes that no longer fit your history.
Common signals:
- Exercise intolerance lasting over 24 hours: A training session that used to barely challenge you now leaves you depleted for two days.
- Brain fog after meals: Especially after carbohydrate-heavy meals, your head feels heavy. That points to a combined load of insulin resistance and mitochondrial weakness.
- Cold hands and feet despite a warm environment: Mitochondria produce heat. When their efficiency drops, peripheral tissues cool faster.
- Fragmented sleep despite tiredness: In particular waking between 2 and 4 am, often with a racing heart. Low progesterone and mitochondrial strain reinforce each other.
- Early muscle fatigue: Climbing stairs feels like a workout, a laundry basket feels heavy, and your legs go heavy on longer walks.
- Slow wound healing and slow recovery from infections: Both require mitochondrial reserve capacity.
None of these symptoms is diagnostic in isolation. But if three or four of them fit and you no longer recognise yourself, that is a concrete signal to take cellular energy seriously rather than treating the situation as a purely hormonal problem.
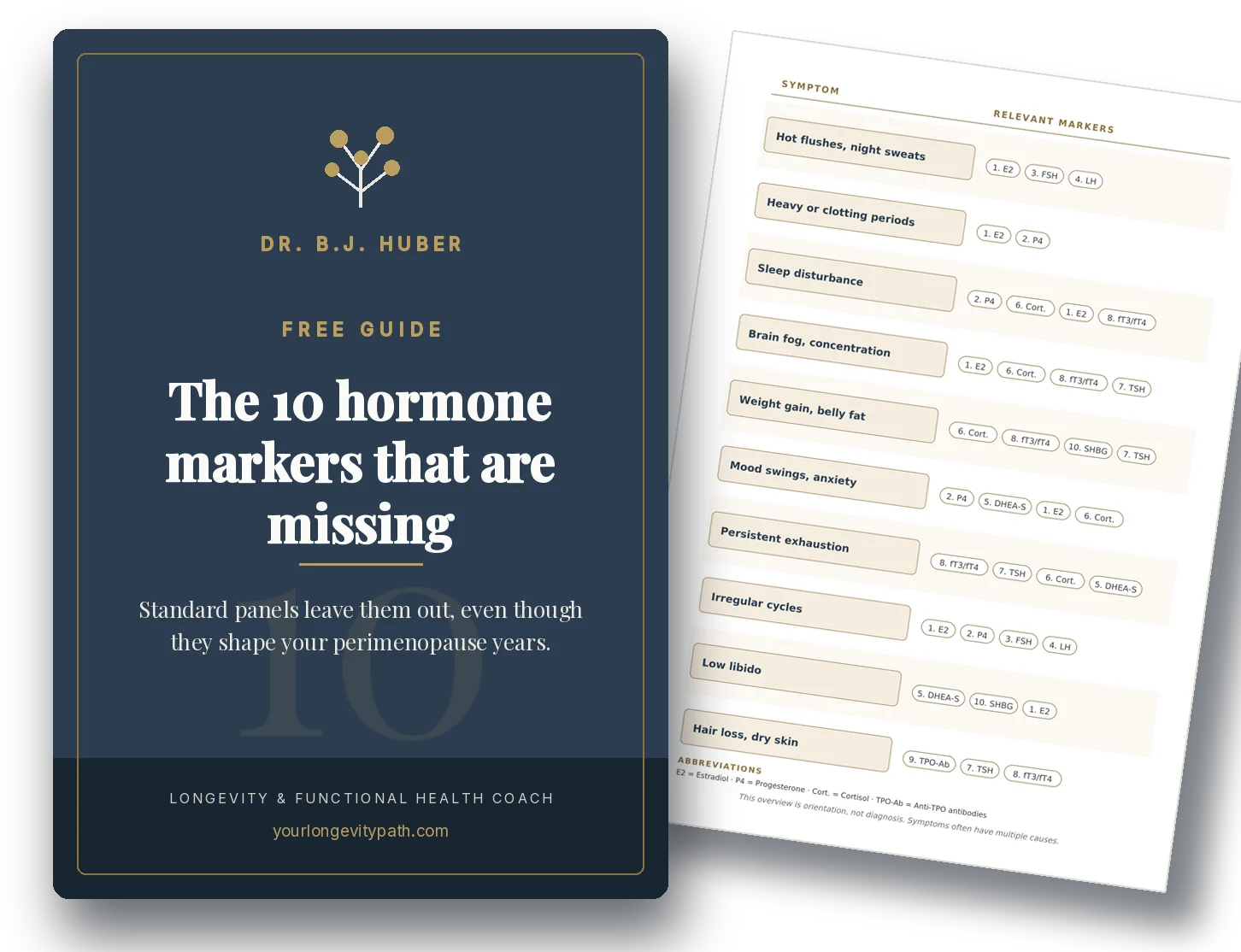
Which blood markers point to mitochondrial strain?
There is no single “mitochondrial test” available in primary care. But several standard markers, viewed together, give a useful overall picture of whether your cellular energy is under pressure.
Worth including in an extended panel:
- Lactate at rest and after moderate exertion: Elevated resting lactate can point to limited aerobic capacity.
- Homocysteine: Reflects B-vitamin status and methylation, both directly tied to mitochondrial function. Functionally optimal: below 8 µmol/l.
- Free T3: The thyroid regulates mitochondrial activity directly. Low free T3 with a normal TSH can amplify a mitochondrial component.
- Ferritin: Iron is a building block of the respiratory chain. Functionally optimal: 50–100 ng/ml.
- Magnesium (in erythrocytes, not serum): Magnesium is a cofactor for over 300 enzymes, many of them in ATP production.
- CoQ10 (ubiquinone) and carnitine: Available in specialised labs, usually out-of-pocket.
For the standard blood markers worth tracking in perimenopause beyond a basic hormone panel, see our overview here.
What can you do to support your mitochondria?
Mitochondria are trainable. At any age. The following levers have the strongest evidence for mitochondrial biogenesis and quality, and they work together, not in isolation.
1. Strength training plus short intervals. A systematic review on exercise physiology shows that high-intensity intervals (HIIT) stimulate mitochondrial biogenesis more strongly than steady-state Zone 2 endurance work. Both have a place, but if you want efficient mitochondrial adaptation, two to three short interval sessions per week (4×4 minutes or 6×1 minute with recoveries) plus two strength sessions deliver the most signal per hour invested (Bishop et al., 2025).
2. Distribute protein across the day. Women over 40 generally need more protein than current dietary reference values suggest (around 1.4–1.8 g per kg body weight) and, importantly, distributed evenly across the day. Three meals with 30 g of protein each stimulate mitochondrial biogenesis in muscle more effectively than the same total amount eaten at one sitting.
3. Prioritise sleep quality. Mitochondria repair during deep sleep. Chronic sleep under six hours, or fragmented sleep, blocks exactly the window in which mitochondrial renewal happens. In perimenopause, consistent bed and wake times, a cool bedroom, no caffeine after 2 pm and, where indicated, a check of progesterone and thyroid function all support sleep architecture.
4. Micronutrient base. The main cofactors for the respiratory chain are magnesium, B vitamins (especially B1, B2, B3, B6, folate and B12), coenzyme Q10 and omega-3 fatty acids. A practical baseline of magnesium-rich foods (pumpkin seeds, nuts, dark leafy greens), B-vitamin sources (eggs, whole grains, legumes) and omega-3 from oily fish or a high-quality algal oil covers a large part of this. Where deficits exist, targeted supplementation can help, but only on the basis of blood markers, not guesswork.
5. Heat and cold exposure. Regular sauna sessions (two to four times per week, 15–20 minutes at 80–90 °C) activate heat shock proteins and stimulate mitochondrial biogenesis. Cold exposure (short cold finishes to your shower, 30–60 seconds) activates brown adipose tissue, which is particularly mitochondrial-dense. Neither is mandatory, but both are well-researched, low-barrier tools.
What stands out: these are the same levers that slow biological ageing. Mitochondrial health and longevity are, at the core, the same question phrased two ways.
Where to go from here
Perimenopause is not a passive phase you have to wait out. It is a window in which many dials respond particularly sensitively, for better or worse. When your cellular energy drops, that is information, not a verdict. Mitochondria respond to training at any age.
If you recognise yourself in these symptoms and want to map out the bigger picture, without juggling supplements, hormones and training plans on your own, you can book a free initial consultation. We will look at where your strongest levers are and which order makes sense for your specific situation.
Scientific sources
-
Levine, M. E., Lu, A. T., Chen, B. H., et al. (2016). Menopause accelerates biological aging. Proceedings of the National Academy of Sciences, 113(33), 9327–9332. doi: 10.1073/pnas.1604558113
-
Yu Y, Yapeng H, Liu Z, Fang L, Li J, Luan Y, Li W, Cong H, Wu X. Mitochondrial dysfunction in perimenopausal mood disorders: From hormonal shifts to neuroenergetic failure (Review). Int J Mol Med. 2025;56:215. doi:10.3892/ijmm.2025.5656 · PMC12513434
-
Mosconi, L., Berti, V., Quinn, C., et al. (2017). Perimenopause and emergence of an Alzheimer’s bioenergetic phenotype in brain and periphery. PLOS ONE, 12(10), e0185926. doi: 10.1371/journal.pone.0185926
-
Yin, F., Yao, J., Sancheti, H., et al. (2015). The perimenopausal aging transition in the female rat brain: decline in bioenergetic systems and synaptic plasticity. Neurobiology of Aging, 36(7), 2282–2295. doi: 10.1016/j.neurobiolaging.2015.03.013
-
Yoshino, M., Yoshino, J., Kayser, B. D., et al. (2021). Nicotinamide mononucleotide increases muscle insulin sensitivity in prediabetic women. Science, 372(6547), 1224–1229. doi: 10.1126/science.abe9985
-
Morifuji M, Higashi S, Ebihara S, Nagata M. Ingestion of β-nicotinamide mononucleotide increased blood NAD levels, maintained walking speed, and improved sleep quality in older adults in a double-blind randomized, placebo-controlled study. GeroScience. 2024;46:4671–4688. doi:10.1007/s11357-024-01204-1
-
Arjmand, B., et al. (2024). Regulation of mitochondrial dysfunction by estrogens and estrogen receptors in Alzheimer’s disease: A focused review. Basic & Clinical Pharmacology & Toxicology. doi: 10.1111/bcpt.14035
-
Bishop DJ, Lee MJ-C, Picard M. Exercise as Mitochondrial Medicine: How Does the Exercise Prescription Affect Mitochondrial Adaptations to Training? Annu Rev Physiol. 2025. doi:10.1146/annurev-physiol-022724-104836
Does menopause really accelerate biological ageing?
Yes. The 2016 study by Levine and colleagues analysed over 3,000 women and found that menopause significantly accelerates epigenetic ageing in blood. Earlier menopause and a longer time since the final menstrual period were both linked to higher biological age acceleration.
What can I do about mitochondrial fatigue in perimenopause?
The strongest levers are strength training combined with short high-intensity intervals, adequate protein at every meal, consistent sleep, regular sauna or heat exposure, and a solid micronutrient base of magnesium, B vitamins and omega-3 fatty acids. All of these support mitochondrial biogenesis and mitophagy.
Do NAD+ boosters like NMN or NR help in perimenopause?
Clinical trials consistently show that both NMN and NR raise NAD+ levels in blood. Functional effects are less clear-cut: one trial in postmenopausal women with prediabetes improved muscle insulin sensitivity, while studies on cognition, fatigue and cardiovascular endpoints show mixed results. The evidence is not yet strong enough to recommend NAD+ boosters across the board.
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.