Hormones
Burnout or Perimenopause? How to Tell What's Actually Wrong
13 May 2026 · By Dr. B.J. Huber · 9 min read
You sleep eight hours, get up, and feel like you never slept at all. By the afternoon your concentration drops, you forget appointments you would never normally miss. People around you say: “You need a break.” Your doctor says: “Sounds like burnout.” And you think: maybe they are right.
But then you take time off, go away for a week, and nothing changes. You sleep ten hours and still wake up drained. The exhaustion follows you no matter how much you rest. This is not burnout. At least not entirely.
What many women between 38 and 50 experience is a collision of two forces: perimenopause destabilises the stress axis while professional and family demands are peaking at the same time. The symptoms look like burnout. But the cause runs deeper. And as long as nobody names that cause, the exhaustion keeps going in circles.
- Perimenopause and burnout share nearly identical symptoms (exhaustion, sleep problems, brain fog, irritability) but require different approaches. The critical difference: hormonal exhaustion does not improve with rest alone.
- Declining oestrogen destabilises the HPA axis (stress axis). At the same time, allopregnanolone, a progesterone metabolite that calms the brain through GABA receptors, drops sharply. The result is heightened stress sensitivity and disrupted sleep.
- In a Dutch Lifelines study of 9,942 women, those with more severe menopause symptoms had 4.5 times greater odds of needing high recovery time after work (Loef et al., 2025).
- Women with ADHD are additionally affected: declining oestrogen worsens the already impaired dopamine function, amplifying exhaustion and concentration difficulties.
Why does perimenopause look so much like burnout?
Perimenopause and burnout affect the same systems: sleep, stress regulation, concentration, and emotional resilience. Fatigue, irritability, brain fog, sleep disruption, feeling overwhelmed: all of these occur in both conditions. That is why they are confused so often.
But the mechanisms differ. Burnout develops through chronic overload that depletes psychological recovery capacity. Perimenopause, by contrast, changes the biological foundation of stress processing itself. Declining hormone levels directly affect cortisol regulation, sleep architecture, and neurotransmitter balance. You are not exhausted because you are doing too much. You are exhausted because your body can no longer buffer stress the way it could at 30.
And here lies the real problem: the two conditions are not mutually exclusive. In a cross-sectional study of nurses, menopausal symptoms were significantly associated with emotional exhaustion (Converso et al., 2019). The hormonal transition increases vulnerability to burnout, and burnout worsens hormonal symptoms. A vicious cycle that nobody breaks as long as only one side is being treated.
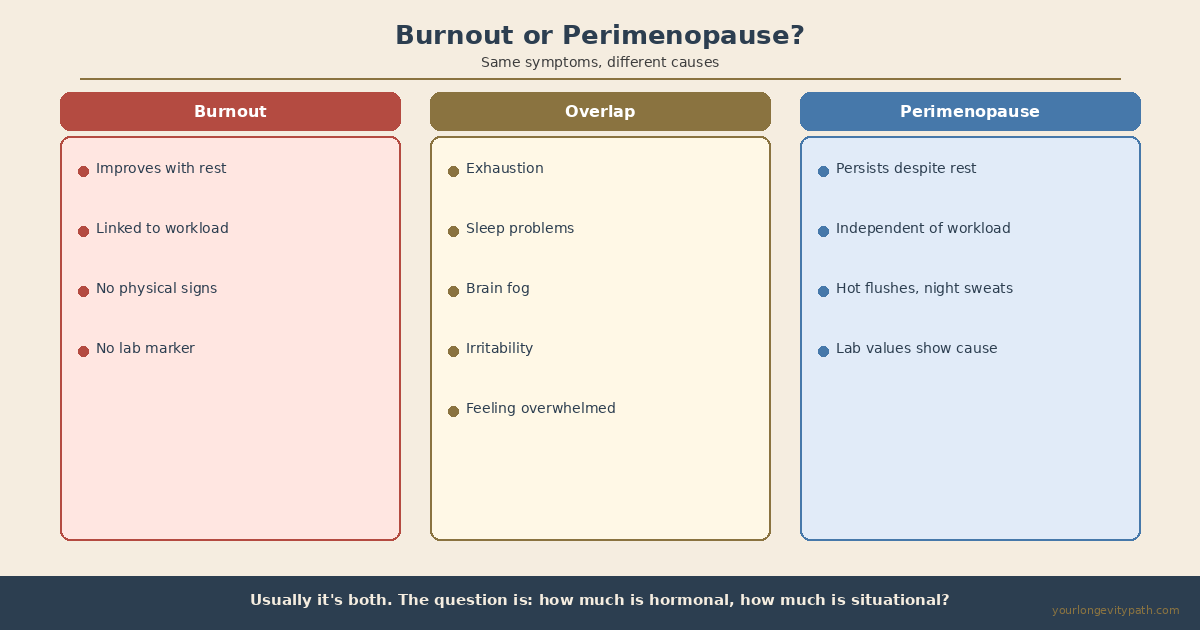 Fig. 1: Burnout and perimenopause share nearly identical symptoms. The critical difference: hormonal exhaustion does not improve with rest alone.
Fig. 1: Burnout and perimenopause share nearly identical symptoms. The critical difference: hormonal exhaustion does not improve with rest alone.
What happens to the HPA axis during perimenopause?
The HPA axis (hypothalamic-pituitary-adrenal axis) is the body’s central stress system. It regulates how much cortisol is released and ensures that the stress response winds down after the threat has passed. Oestrogen plays a key role: it prevents the HPA axis from overactivating and keeps the cortisol response in balance (Gordon et al., 2015).
When oestrogen declines in perimenopause, the HPA axis loses that buffer. The cortisol response becomes more reactive, the stress reaction more intense, and the feedback loop (which normally brings cortisol back down after a challenge) works less effectively. Oestradiol fluctuations are directly linked to elevated cortisol levels and negative mood, particularly in women with a history of depression (Gordon et al., 2015; Hantsoo et al., 2023).
What this means in practice: the same workload, the same family demands you handled comfortably at 35 can suddenly feel overwhelming at 42. Not because you have become weaker, but because the hormonal foundation of your stress resilience has shifted.
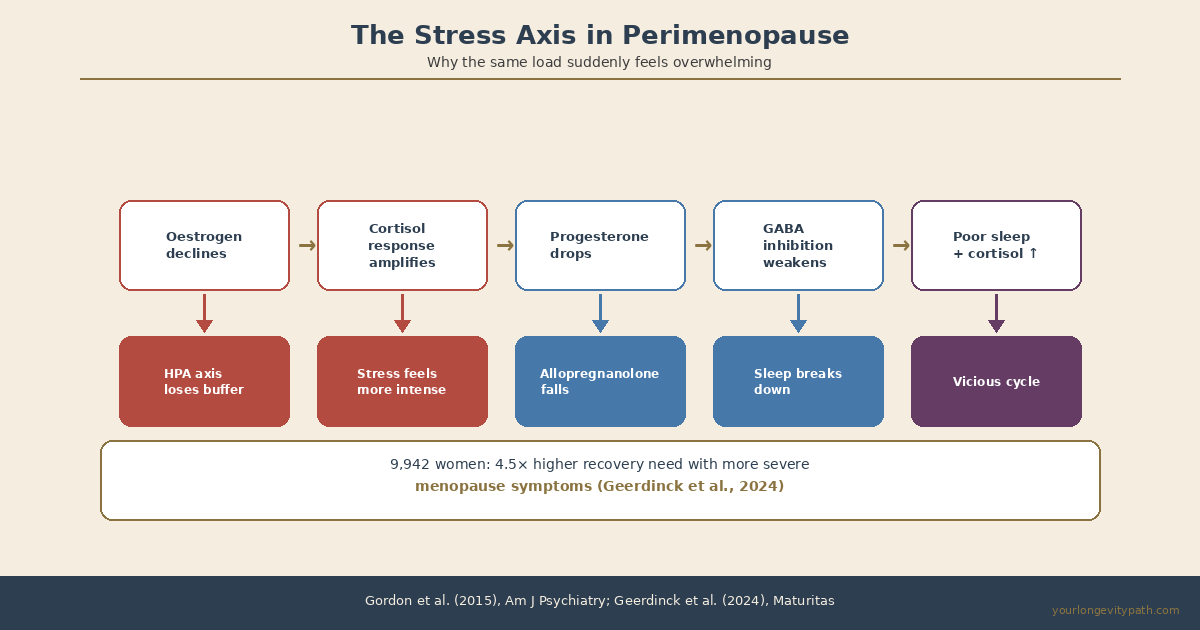 Fig. 2: Declining oestrogen and progesterone destabilise the HPA axis and GABAergic inhibition simultaneously, creating a vicious cycle of heightened stress sensitivity and disrupted sleep (Gordon et al., 2015; Hantsoo et al., 2023).
Fig. 2: Declining oestrogen and progesterone destabilise the HPA axis and GABAergic inhibition simultaneously, creating a vicious cycle of heightened stress sensitivity and disrupted sleep (Gordon et al., 2015; Hantsoo et al., 2023).
Why does your sleep break down even though you are exhausted?
Progesterone is more than a reproductive hormone. In the brain, it is converted into allopregnanolone, a neurosteroid that modulates GABA-A receptors. GABA is the brain’s primary inhibitory neurotransmitter: it dampens neural overactivity and promotes relaxation and sleep. Allopregnanolone acts on the same receptors as benzodiazepines, only naturally (Gordon et al., 2015).
During perimenopause, progesterone often drops before oestrogen does. As it falls, so does allopregnanolone, and GABAergic inhibition in the brain weakens. The result: you are stuck in a low-grade state of alert. Falling asleep becomes harder, staying asleep becomes fragile, and those classic 3 a.m. wake-ups where you lie there with a racing heart are a hallmark sign.
A meta-analysis found that sleep disorders among postmenopausal women (when progesterone is at its lowest) exceed 50%. Poor sleep is not just a symptom; it amplifies everything else. Cortisol regulation suffers, stress sensitivity increases, and cognitive performance drops. When sleep breaks down, you do not just feel tired; you become hormonally less stable.
How can you tell burnout apart from hormonal exhaustion?
The symptoms overlap substantially, but there are differences that can bring clarity.
- Does rest actually help? With burnout, a real holiday or extended time off brings noticeable improvement. With hormonal exhaustion, the fatigue persists regardless of how much you rest.
- Are there physical symptoms alongside the fatigue? Hot flushes, night sweats, cycle changes, and vaginal dryness are perimenopause signs that do not occur with burnout.
- When did the exhaustion begin? Burnout builds over months to years and is clearly tied to specific stressors. Hormonal exhaustion can creep in gradually without any change in external demands.
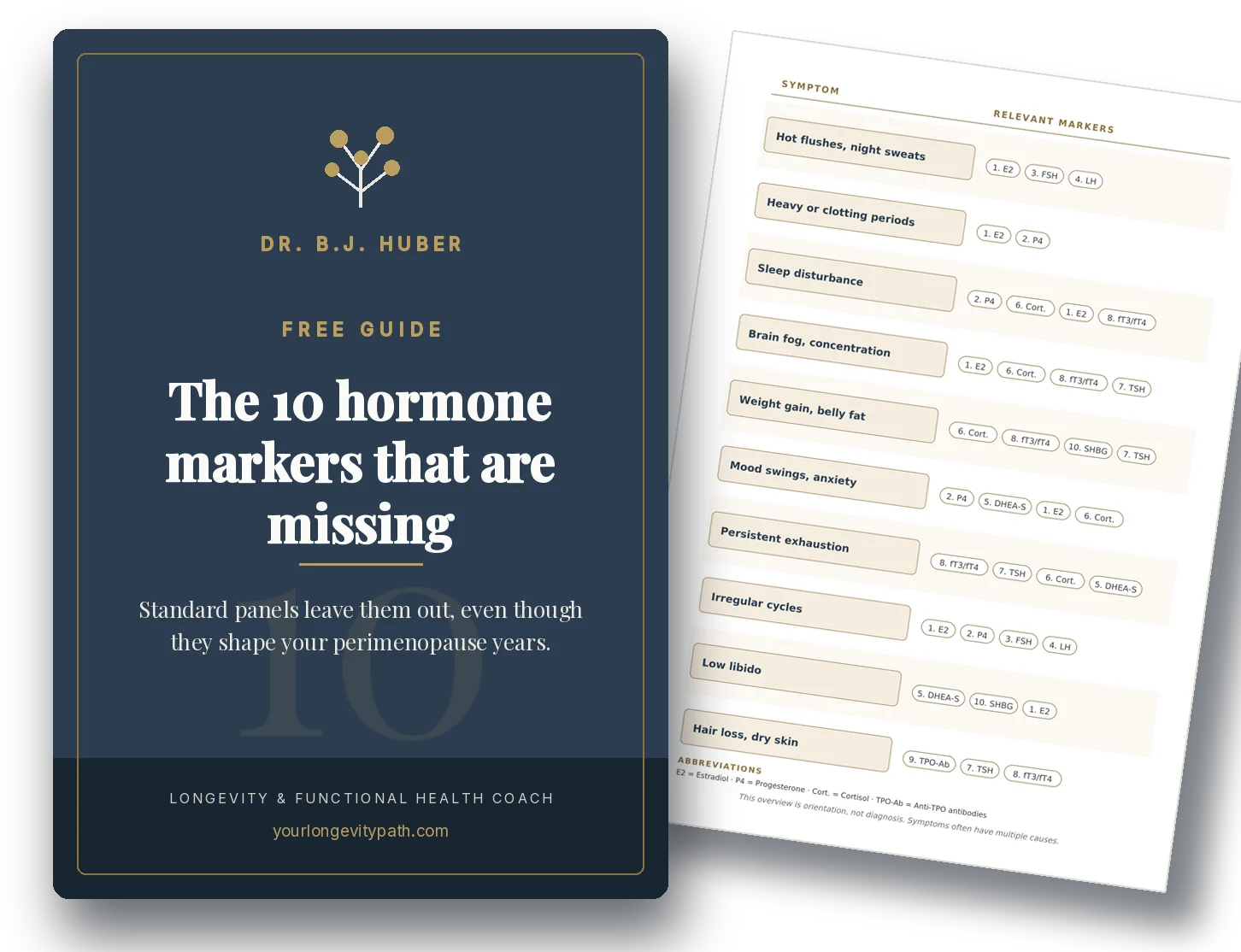
- What do the lab values show? Burnout leaves no specific lab markers (though cortisol dysregulation may appear). Hormonal causes show up through FSH, oestradiol, progesterone, thyroid markers (TSH, free T3), ferritin, and vitamin D. You can find the complete list with optimal ranges in my article on lab values in perimenopause.
The key insight: the question is not “burnout or hormones?” but “how much of my exhaustion is hormonal, and how much is situational?” Most of the time, it is both.
Another factor that often gets overlooked: women with ADHD are particularly affected during perimenopause. Oestrogen supports dopamine production in the prefrontal cortex, precisely the brain region that is already underserved in ADHD. As oestrogen declines, dopamine function deteriorates further. In an Icelandic cohort study, women with ADHD reported severe perimenopausal symptoms at nearly double the rate (Jakobsdóttir Smári et al., 2025). I will be covering this connection in a dedicated article.
What helps when 41% of working women need high recovery time?
In a Belgian cross-sectional study of 760 working menopausal women, the prevalence of a high need for recovery after work was 41.2%. Among those who experienced work-related problems from menopausal symptoms, the rate was 61.1% (Kiss et al., 2024). In a larger Dutch Lifelines cohort of 9,942 peri- and postmenopausal women, every 10-point increase in menopause symptom score (Greene Climacteric Scale) raised the odds of high recovery need by a factor of 4.5 (Loef et al., 2025).
These numbers make one thing clear: the exhaustion is neither imaginary nor a sign of weakness. It is a predictable consequence of hormonal changes that affects nearly half of all working women in this life phase.
What you can do:
Get your hormonal status checked: Request comprehensive lab work that goes beyond the basics. FSH, oestradiol, and progesterone alone are not enough. Ferritin, thyroid markers (TSH, free T3, TPO antibodies), vitamin D, cortisol, and fasting insulin should be included. You can find the full list in my lab values article.
Prioritise sleep as a hormonal necessity: Not as a lifestyle tip, but as a biological requirement. Fixed sleep and wake times, no blue light after 8 p.m., a cool bedroom (18–19°C). Progesterone plays a central role; discuss with your doctor whether support may be appropriate.
Stabilise your stress axis: The HPA axis needs more deliberate regulation during perimenopause. Breathing exercises (six breaths per minute), regular movement (strength training plus moderate endurance), and time in nature all lower cortisol measurably and support stress resilience.
Reassess your load honestly: When biological buffer capacity shrinks, external demands need to be adjusted. This is not a step backwards; it is the logical consequence.
Two causes, one exhaustion
Exhaustion in your forties rarely has a single cause. Perimenopause destabilises the stress axis, disrupts sleep, and shifts neurotransmitter balance. At the same time, many women in this phase face peak professional and family pressure. The two factors reinforce each other, and as long as only one is addressed, the cycle continues.
The first step is to look at both sides. Not burnout or hormones, but both. With the right lab work, an honest assessment of your load, and targeted measures for sleep and stress regulation, the vicious cycle can be broken.
If you would like to find out where you stand and which levers would make the biggest difference for you, a free initial consultation is a good starting point.
Scientific references
- Gordon, J.L. et al. (2015). Ovarian Hormone Fluctuation, Neurosteroids and HPA Axis Dysregulation in Perimenopausal Depression: A Novel Heuristic Model. Am J Psychiatry, 172(3), 227–236. doi: 10.1176/appi.ajp.2014.14070918
- Converso D, Viotti S, Sottimano I, Loera B, Molinengo G, Guidetti G. The relationship between menopausal symptoms and burnout. A cross-sectional study among nurses. BMC Women’s Health. 2019;19:148. doi:10.1186/s12905-019-0847-6 · PMID:31775724
- Kiss P, Depypere H, De Meester M, Vingerhoets I, Van Hoecke M, Braeckman L. Need for recovery after work and associated risk factors in working menopausal women. Maturitas. 2024;187:108054. doi:10.1016/j.maturitas.2024.108054 · PMID:38905864
- Loef B et al. Lifestyle behaviors do not moderate the association between menopausal symptoms and need for recovery after work. Maturitas. 2025;203:108757. PMID:41172717
- Jakobsdóttir Smári U et al. Perimenopausal symptoms in women with and without ADHD: A population-based cohort study. European Psychiatry. 2025. doi:10.1192/j.eurpsy.2025.10101 · PMC12538516
- Hantsoo L, Jagodnik KM, Novick AM, Baweja R, Lanza di Scalea T, Ozerdem A, McGlade EC, Simeonova DI, Dekel S, Kornfield SL, Nazareth M, Weiss SJ. The role of the hypothalamic-pituitary-adrenal axis in depression across the female reproductive lifecycle: current knowledge and future directions. Front Endocrinol. 2023;14:1295261. doi:10.3389/fendo.2023.1295261 · PMID:38149098
How do I tell the difference between burnout and perimenopause?
Burnout improves with genuine rest, such as a real holiday or extended time off. Hormonal exhaustion persists regardless of how much you sleep. Physical signs like hot flushes, night sweats, and cycle changes point to perimenopause, not burnout. Lab work (cortisol, FSH, oestradiol, ferritin, thyroid panel) can clarify the underlying cause.
Why are women over 40 more vulnerable to burnout?
During perimenopause, declining oestrogen and progesterone destabilise the HPA axis (stress axis). At the same time, levels of allopregnanolone, a progesterone metabolite that calms the brain through GABA receptors, drop sharply. The result is heightened stress sensitivity, disrupted sleep, and faster exhaustion.
Which lab values help clarify the cause of exhaustion?
A comprehensive panel should include FSH, oestradiol, progesterone, TSH, free T3, TPO antibodies, ferritin, vitamin D, cortisol, and fasting insulin. Standard testing often only covers FSH and oestradiol, which is not enough to distinguish hormonal from situational exhaustion.
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.