ADHD
Why ADHD symptoms intensify in perimenopause
20 May 2026 · By Dr. B.J. Huber · 12 min read
You always managed somehow. Lists, alarms, a good memory for what mattered, maybe a bit more effort than other people needed, but it worked. And then, somewhere around 40, it stopped working. Appointments slip through, words vanish mid-sentence, your mind jumps from one open tab to the next, and the smallest thing throws you off emotionally. You wonder whether you are losing your mind.
You are not. What many women experience in this phase has a biological basis that has only been well described in recent years: the hormones that helped regulate your brain for decades fall out of rhythm in perimenopause. For women with an ADHD predisposition, diagnosed or not, this shift lands on an already sensitive system. The result can feel like a sudden loss of your own ability to function.
What makes it especially unsettling is that it often begins gradually and then hits a breaking point. First it is just the odd forgotten appointment, then they pile up. First only occasional irritability, then the feeling of being permanently on the edge of overflowing. Many women put it down to stress, too little sleep or simply getting older, until they reach the point where their tried-and-tested strategies no longer work. That is exactly the point where it pays to look behind the symptoms.
This article is about the two hormone axes at the heart of this: oestrogen and dopamine on one side, progesterone and the calming GABA neurotransmitter on the other. And about what current research says, without making diagnoses or promising cures.
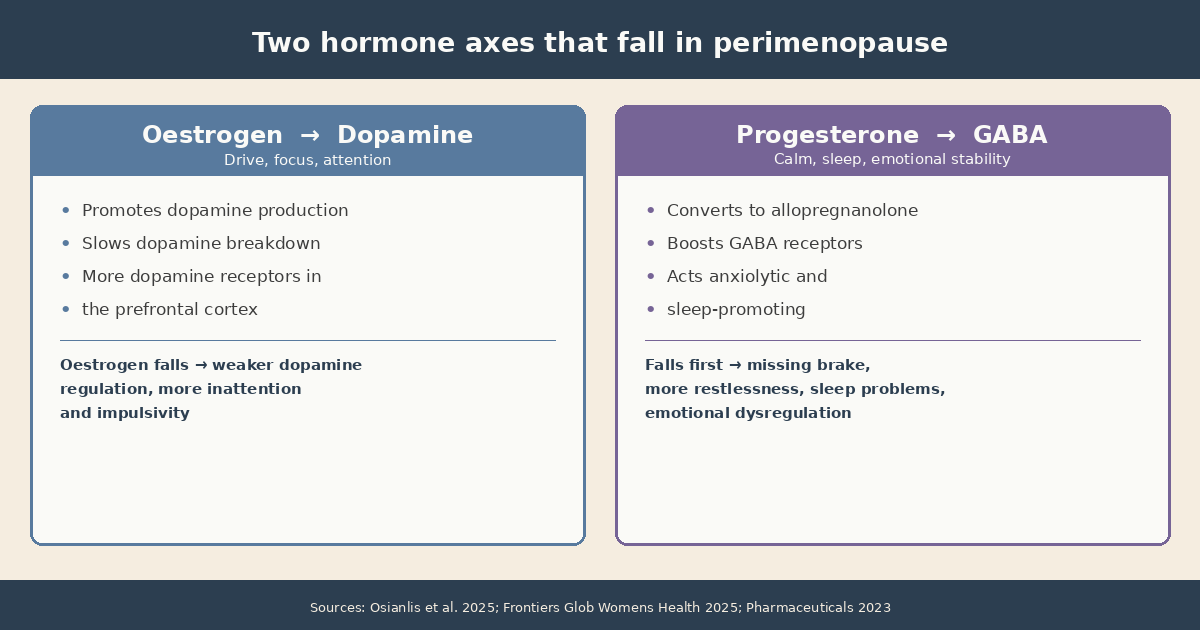
- Oestrogen supports dopamine function in the prefrontal cortex, the brain region for attention and self-regulation. When oestrogen falls in perimenopause, the dopamine shortfall in ADHD can intensify.
- Progesterone often falls first. Through its metabolite allopregnanolone, it boosts the calming GABA neurotransmitter. When it drops, a natural brake on restlessness and disturbed sleep is lost.
- A 2025 population study (n=5,392) found that women with ADHD experience more severe perimenopausal symptoms, often earlier than women without ADHD (Jakobsdóttir Smári et al., 2025).
Why do ADHD symptoms often get stronger in perimenopause?
Because the hormones that helped stabilise the brain for decades fluctuate and decline in perimenopause. With an ADHD predisposition, this loss lands on an already sensitive attention and regulation system, and the symptoms become more pronounced.
A 2025 systematic review summarised the evidence: in women with ADHD, mood and cognition shift markedly across hormonal life stages, and phases of rapid oestrogen decline frequently coincide with a worsening of core symptoms (Osianlis et al., 2025). Perimenopause is the longest and most intense of these decline phases.
A 2025 population-based study examined 5,392 women aged 35 to 55. Women with ADHD had higher perimenopausal symptom scores than women without ADHD, reported severe symptoms more often, and tended to be affected earlier (Jakobsdóttir Smári et al., 2025). Importantly, this study describes an association, not a cause-and-effect chain for any individual.
The feeling of suddenly no longer functioning is therefore neither imagination nor failure. It is the consequence of a biological shift that research is only now beginning to map.
What does oestrogen have to do with dopamine and attention?
Oestrogen supports dopamine function directly. It promotes dopamine production, slows its breakdown and increases the density of dopamine receptors in the prefrontal cortex, the brain region that governs attention, working memory and impulse control.
ADHD is, at its core, a matter of dopamine regulation. The brain needs dopamine to sustain attention, prioritise tasks and regulate emotion. If oestrogen supports dopamine function, then a falling oestrogen level also means weaker dopamine regulation. This is exactly what research describes for phases of rapid oestrogen decline (Frontiers in Global Women’s Health, 2025).
The link is already visible across the menstrual cycle: a 2026 review showed that cycle-related oestrogen fluctuations in women with ADHD measurably coincide with changes in mood and cognitive performance, especially in the late luteal phase when oestrogen drops (Menstrual Cycle-Related Hormonal Fluctuations in ADHD, 2026). Perimenopause is essentially the same mechanism, stretched over years and without the monthly rebound.
The emotional component is especially striking. Dopamine governs not only attention but also how strongly we react to reward, rejection and frustration. When dopamine regulation weakens, many women report a noticeably shorter fuse, deeper mood dips and heightened sensitivity to criticism. This emotional dysregulation is a core feature of ADHD and is frequently amplified by the hormonal shift. Women who once shrugged off conflict and setbacks often experience them as overwhelming in perimenopause, without anything in the external situation having changed.
For how the perimenopausal energy drop plays out at the cellular level, see our detailed article here.
What role does progesterone play, the hormone that often falls first?
Progesterone often falls first in perimenopause, years before oestrogen declines noticeably. In the body it converts into allopregnanolone, a compound that boosts the calming neurotransmitter GABA. When progesterone drops, this natural brake on inner restlessness is lost.
Allopregnanolone binds to the GABA-A receptors in the brain and acts there much like an anti-anxiety medication: anxiolytic, sleep-promoting and mood-stabilising (Pharmaceuticals, 2023). As long as there is enough progesterone, there is a constant calming effect in the background. When progesterone falls, this GABA effect weakens, and the brain stays in a state of heightened excitability.
For women with ADHD this matters twice over. Emotional dysregulation, inner restlessness and sleep problems are already among the most burdensome features of ADHD. When the GABA brake weakens, these very symptoms can intensify. A review describes that progesterone and its metabolites play an important role in affect regulation in the female brain, and that their loss is linked to disturbed sleep, anxiety and mood swings (Allopregnanolone and Reproductive Psychiatry, 2019).
This early drop in progesterone explains why many women report lying awake at night, palpitations and a shorter fuse in early perimenopause, often before classic menopausal symptoms such as hot flushes set in.
Why do perimenopause and ADHD reinforce each other?
Because the two escalate in a feedback loop. This is not a single isolated problem but a chain reaction that keeps the brain under constant stress:
- Sleep suffers: The early progesterone drop disturbs night-time rest and impairs recovery.
- The control centre tires: Sleep deprivation hits the prefrontal cortex hard, the very region already under pressure in ADHD.
- Executive function weakens: The result is more forgetfulness, weaker impulse control and noticeably less stress tolerance in daily life.
- The stress hormone rises: Constant overwhelm drives cortisol levels up.
- The loop closes: Chronically high cortisol further degrades sleep and dopamine efficiency. It all starts again, only more intense.
On top of this vicious cycle comes the loss of compensation. Many women with ADHD hold their daily lives together for years through constant self-monitoring, lists and enormous mental effort. This unconscious masking takes a great deal of energy. When hormones, sleep and stress regulation all decline at once, there is simply no longer enough left for this compensation. The painstakingly maintained system becomes visibly unstable.
Current reviews of female ADHD describe exactly this interplay: hormonal transitions worsen both ADHD symptoms and mood disturbances, while tailored treatment approaches are still lacking (Frontiers in Global Women’s Health, 2025).
This explains why midlife feels like a double storm for many affected women. It is not a weakness to need more support in this phase than before, but the logical consequence of a system buckling under the added load.
Why are many women only diagnosed with ADHD now?
Many women compensated for their ADHD for decades, partly supported by the higher oestrogen levels of their fertile years. When that hormonal support fades in perimenopause, compensation becomes harder, and the symptoms become clearly visible for the first time.
ADHD in girls and women often shows up less as hyperactivity and more as inner restlessness, daydreaming, forgetfulness and a high mental cost to organise daily life. This subtler presentation is frequently missed in childhood. Many women develop elaborate coping strategies over the years and simply consider themselves chaotic or disorganised (Frontiers in Global Women’s Health, 2025).
In perimenopause this fragile balance tips. The familiar strategies stop working, and what was previously seen as a personality trait becomes recognisable as possible ADHD. This explains the striking cluster of first-time ADHD diagnoses in women at midlife. The key point remains: whether ADHD is actually present is always determined by a medical or psychological assessment, not by an online article and not by coaching.
For many women this late realisation is, paradoxically, a relief. Someone who spent decades believing they were simply not disciplined or resilient enough suddenly finds a biological explanation. It reframes how they see their own life in hindsight and lifts part of the self-criticism that has built up over the years. What matters is translating this insight into concrete, achievable steps rather than letting it turn into new pressure. It is not about pinning on yet another label, but about understanding your own brain better and supporting it accordingly.
How do you tell ADHD apart from perimenopausal brain fog?
In an individual case this is difficult, because the symptoms overlap heavily. Both involve concentration problems, forgetfulness and word-finding difficulties. A few patterns can help with seeing the bigger picture, without replacing a diagnosis.
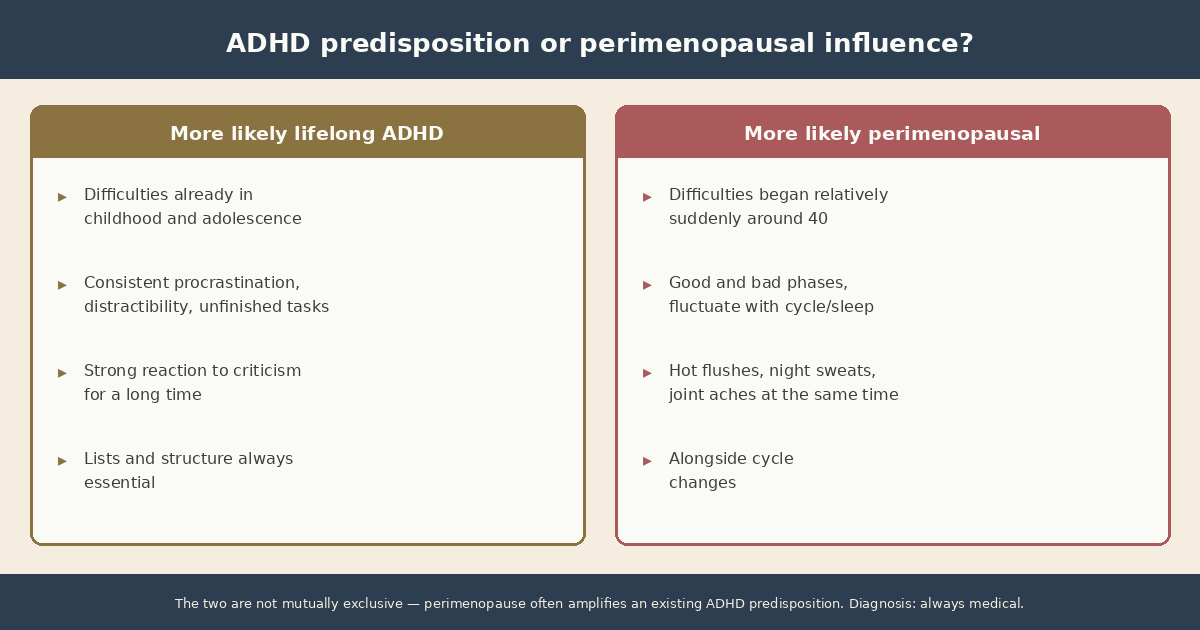
Signs that point more towards a lifelong ADHD predisposition:
- The difficulties existed in milder form in childhood and adolescence, not only from 40 onwards.
- There is a consistent pattern of procrastination, distractibility and trouble finishing tasks.
- Strong emotional reactions to rejection or criticism have been with you for a long time.
- Structures, lists and external reminders were always essential, not just recently.
Signs that point more towards a perimenopausal influence:
- The difficulties began relatively suddenly around 40, alongside cycle changes, sleep problems or hot flushes.
- There are good and bad phases that fluctuate with your cycle or your sleep.
- Hot flushes, night sweats or joint aches appear at the same time.
In reality, the two are not mutually exclusive. Very often perimenopause amplifies a pre-existing, previously well-compensated ADHD predisposition. It is precisely this combination that makes the picture complex and a careful medical assessment all the more valuable.
What can you do to support your brain?
Regardless of whether an ADHD diagnosis is eventually made, there are lifestyle levers that demonstrably support dopamine and GABA function. They do not replace a medical assessment or any treatment, but they can strengthen the foundation.
1. Protein at breakfast. Dopamine is made from the amino acid tyrosine, found in protein-rich foods. A protein-rich breakfast with eggs provides the building blocks for dopamine production early in the day, when focus matters most.
2. Movement as a dopamine lever. Physical activity acutely raises dopamine and noradrenaline availability in the brain. Even a brisk walk or a short strength session before a focus-heavy task can improve concentration. Regular training also works through cellular energy.
3. Prioritise sleep. Sleep deprivation worsens attention and emotional regulation in everyone, and especially in ADHD. Since the progesterone drop disturbs sleep anyway, consistent bed and wake times, a cool bedroom and avoiding afternoon caffeine are particularly effective.
4. Reduce input deliberately. When the internal brake weakens, external structure helps: fewer open tabs, one task at a time, clear lists and quiet work blocks without notifications. This relieves a brain that currently has less filtering capacity.
5. Keep an eye on micronutrients. Iron, vitamin D, omega-3 fatty acids and magnesium are involved in dopamine and GABA function. For the blood markers worth checking in perimenopause, see our overview here. Supplements belong on the basis of blood markers and medical guidance, not guesswork.
6. Actively down-regulate stress. Because stress and lack of sleep feed the vicious cycle of hormone decline and weakened self-regulation, deliberately calming the nervous system pays off. Long, slow exhalations activate the calming branch of the autonomic nervous system, short walks in green spaces measurably lower stress levels, and conscious breaks between tasks stop overwhelm from accumulating across the day. These small micro-pauses cost little time but relieve a regulation system that is already running at its limit in this phase.
Where to go from here
If you recognise yourself in this article, the most important step is not to blame yourself for what is happening biologically in your brain. The intensification of attention and regulation problems in perimenopause is real and scientifically described, not a character flaw.
The right next step depends on your situation. If you suspect ADHD, a specialist medical or psychological assessment is the way to go. If you want to make sense of the bigger picture across hormones, sleep, nutrition and daily structure, and use the lifestyle levers in a targeted way, you can book a free initial consultation. We will look at where your strongest levers are, always within what coaching can do and what belongs in medical hands.
Scientific sources
-
Jakobsdóttir Smári, U., et al. (2025). Perimenopausal symptoms in women with and without ADHD: A population-based cohort study. European Psychiatry. PMC12538516
-
Osianlis, E., Thomas, E. H. X., Jenkins, L. M., & Gurvich, C. (2025). ADHD and Sex Hormones in Females: A Systematic Review. Journal of Attention Disorders. doi: 10.1177/10870547251332319
-
Research advances and future directions in female ADHD: the lifelong interplay of hormonal fluctuations with mood, cognition, and disease. (2025). Frontiers in Global Women’s Health. PMC12277363
-
Menstrual Cycle-Related Hormonal Fluctuations in ADHD: Effect on Cognitive Functioning (A Narrative Review). (2026). Journal of Clinical Medicine, 15(1), 121. doi: 10.3390/jcm15010121
-
Progesterone and Its Metabolites Play a Beneficial Role in Affect Regulation in the Female Brain. (2023). Pharmaceuticals. PMC10143192
-
Allopregnanolone and Reproductive Psychiatry: An Overview. (2019). International Review of Psychiatry. PMC6594874
Can ADHD symptoms get worse in perimenopause?
Yes. A 2025 population-based study (n=5,392) found that women with ADHD experience more severe perimenopausal symptoms and often earlier than women without ADHD. The likely driver is falling oestrogen, which supports dopamine function in the prefrontal cortex.
What role does progesterone play in ADHD during perimenopause?
Progesterone often falls first in perimenopause. It converts into allopregnanolone, which boosts the calming GABA neurotransmitter. When progesterone drops, this natural brake weakens, which can increase restlessness, sleep problems and emotional dysregulation.
Why are so many women only diagnosed with ADHD in perimenopause?
Many women compensated for previously unnoticed ADHD for decades. As oestrogen falls in perimenopause, that compensation becomes harder and symptoms emerge more clearly. A diagnosis is always made by a doctor or psychologist.
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.