ADHD
Magnesium L-Threonate for ADHD: The Only Form That Reaches Your Brain
8 April 2026 · By Dr. B.J. Huber · 11 min read
If you or someone you care about has ADHD, you’ve probably heard the standard advice: “Try magnesium.” But which form? And why does it matter?
Most over-the-counter supplements, whether glycinate, citrate, or oxide, don’t raise brain magnesium levels in meaningful amounts. For ADHD, where the primary dysfunction sits in the prefrontal cortex, a supplement that can’t reach your brain is like offering a pilot a map of a different country.
That’s where magnesium L-threonate (often patented as Magtein®) is different. This is the only form clinically shown to significantly elevate cerebral magnesium concentrations. And for people with ADHD, emerging research suggests it may address both acute symptoms and a hidden problem that stimulant medications don’t solve: the rebound effect.
- Only magnesium L-threonate crosses the blood-brain barrier in therapeutically meaningful amounts — standard forms like citrate or glycinate provide negligible cerebral elevation.
- NMDA receptor blockade by magnesium prevents the glutamate excitotoxicity that drives sensory overload, emotional dysregulation, and medication rebound crashes.
- Pilot studies show 47% of ADHD adults experienced clinically relevant improvements in executive function and attention shifting after 12 weeks at 1.5–2g daily.
Why ADHD and Low Magnesium Go Hand in Hand
The connection between ADHD and this mineral isn’t new. A meta-analysis of seven studies found significantly lower serum magnesium levels in people with ADHD compared to controls, a pattern so consistent it points to a real biological mechanism, not coincidence (Effatpanah et al., 2019). This is just one of several micronutrient imbalances commonly found in ADHD — for a complete picture of what blood values to check, see my full guide on ADHD and micronutrient deficiencies.
The brain runs on three overlapping systems: dopamine for motivation and focus, norepinephrine for alertness, and glutamate for excitation. In ADHD, the prefrontal cortex shows dysregulated glutamatergic signaling, too much excitation, not enough inhibition (Cheng et al., 2017). Magnesium acts as a natural NMDA receptor antagonist, meaning it dampens glutamate’s excitatory drive. Without enough of it, glutamate can run unchecked, leaving the brain in a state of sensory overload and cognitive chaos.
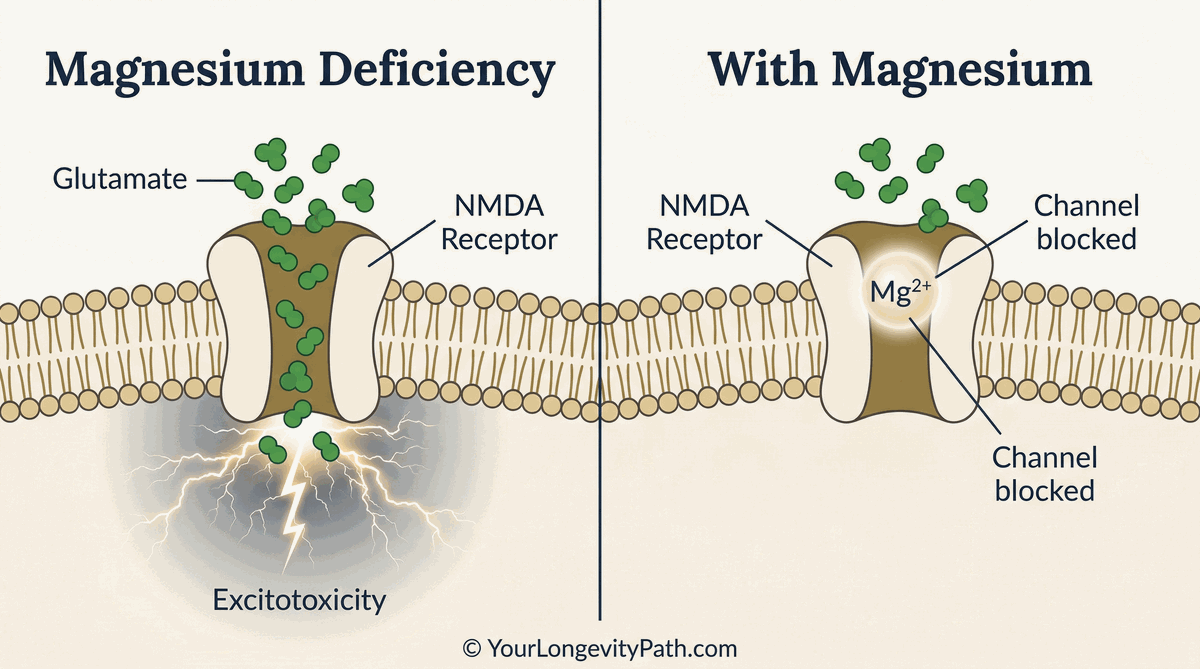 Fig. 1: The NMDA receptor under magnesium deficiency (left) vs. adequate magnesium (right). Without magnesium, glutamate floods the channel unchecked, causing excitotoxicity. With magnesium, the channel is blocked and neural excitation is regulated. © YourLongevityPath.com
Fig. 1: The NMDA receptor under magnesium deficiency (left) vs. adequate magnesium (right). Without magnesium, glutamate floods the channel unchecked, causing excitotoxicity. With magnesium, the channel is blocked and neural excitation is regulated. © YourLongevityPath.com
This is why people with ADHD often struggle with emotional regulation and irritability, sensory sensitivity (sounds, lights, textures feel overwhelming), sleep onset (the brain won’t quiet down), anxiety that spikes without obvious triggers, and the sense of your mind running at 1000 rpm even when you’re trying to rest.
In short: the ADHD brain is already running hot. Low magnesium removes the one brake that could slow down the excitatory spiral.
Magnesium L-Threonate: A Different Mechanism
Most supplements are poorly absorbed and don’t meaningfully raise cerebral concentrations. The threonate form is different. It was specifically designed by MIT researchers to deliver magnesium directly into brain cells (Slutsky et al., 2010).
L-threonic acid is a metabolite of vitamin C (ascorbic acid). It acts as a highly specific carrier molecule, shuttling the magnesium directly across the blood-brain barrier into the central nervous system. This is not passive diffusion; it is an active, carrier-mediated process that standard forms simply cannot replicate.
Once inside, magnesium L-threonate:
Enhances synaptic plasticity. Elevated brain magnesium strengthens connections between neurons, supporting learning and memory consolidation. In the original Slutsky study, animals given this compound showed improved cognitive function and faster acquisition of new tasks.
Stabilizes NMDA signaling. By blocking excessive glutamate activity, it reduces excitatory overload without shutting down the beneficial signaling you need for focus and motivation.
Supports fear extinction. For people with ADHD who also carry trauma or anxiety, elevated brain magnesium enhanced fear extinction in the prefrontal cortex, helping the brain move past threat-detection mode more smoothly (Abumaria et al., 2011).
The carrier molecule itself is biologically active, which is part of why this form has such a pronounced effect on brain function compared to other magnesium supplements.
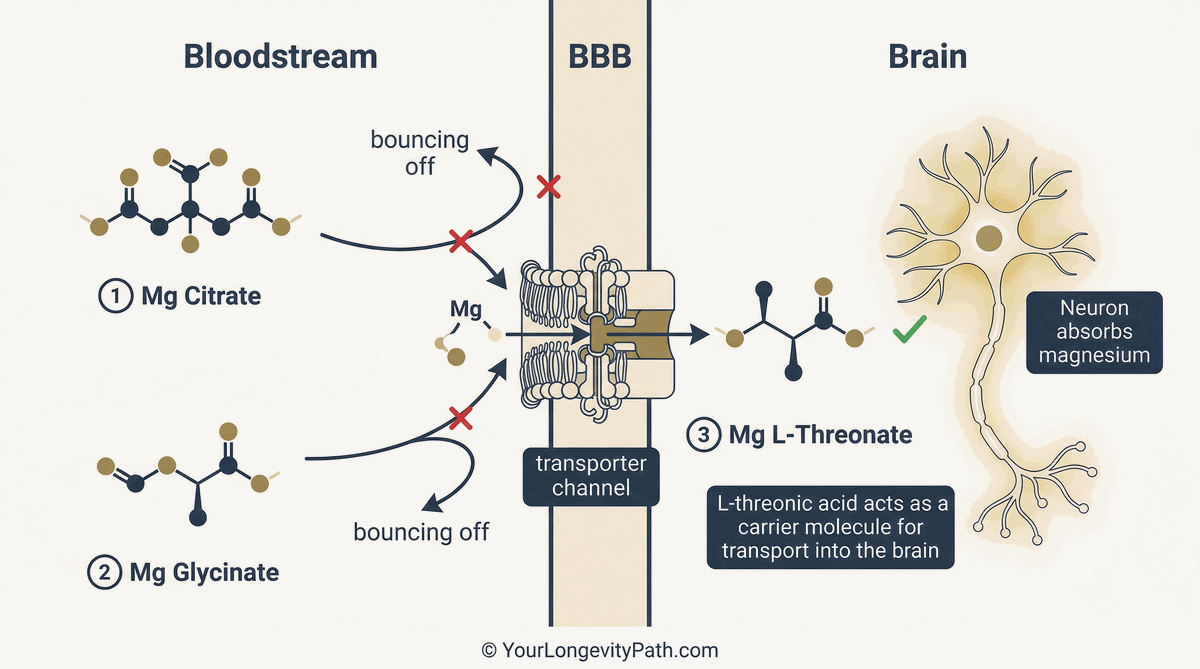 Fig. 2: Why magnesium L-threonate is different: Standard forms like citrate and glycinate cannot efficiently cross the blood-brain barrier. L-threonate uses a specific transporter channel to deliver magnesium directly into the brain. © YourLongevityPath.com
Fig. 2: Why magnesium L-threonate is different: Standard forms like citrate and glycinate cannot efficiently cross the blood-brain barrier. L-threonate uses a specific transporter channel to deliver magnesium directly into the brain. © YourLongevityPath.com
The ADHD-Stimulant-Magnesium Triangle
Here’s where most discussions stop short. If magnesium is so important, why doesn’t research focus on it more?
The answer: stimulant medications (methylphenidate, amphetamine-based compounds) work. They increase dopamine and norepinephrine in the synaptic cleft. For many people, that effect is enough to restore functional focus and executive control. The problem is what happens when the medication wears off.
As the medication clears from your system, neurotransmitter levels drop rapidly. This isn’t a gradual fade; it’s a cliff. The result: a “rebound” period where symptoms temporarily worsen. Irritability, restlessness, emotional dysregulation spike. Some people describe it as feeling like the ADHD is worse off medication than on it. That’s not weakness or drug dependence; it’s neurochemistry. The brain briefly overshoots on the low end, like a pendulum swinging too far.
Recent evidence suggests stimulants also alter magnesium homeostasis. Schmidt et al. (1994) found that both methylphenidate and dextroamphetamine affect the calcium-magnesium ratio in the blood, a sign that these medications may increase magnesium excretion through the kidneys. Over weeks or months, this could contribute to cumulative depletion.
Here’s the plausible chain:
- Stimulant medication wears off, neurotransmitter cliff
- Depleted brain magnesium, reduced NMDA buffering
- Less NMDA blockade, glutamate overactivity spikes
- Result: amplified rebound irritability and restlessness
This is a hypothesis, not proven fact. But the mechanistic pieces fit. And it suggests that adding magnesium L-threonate (Magtein®) might smooth out the rebound transition by maintaining more stable NMDA signaling as medication levels fall.
Stimulants address the dopamine side of ADHD. L-threonate may address the glutamate side. Together, they could provide a more complete neurochemical foundation.
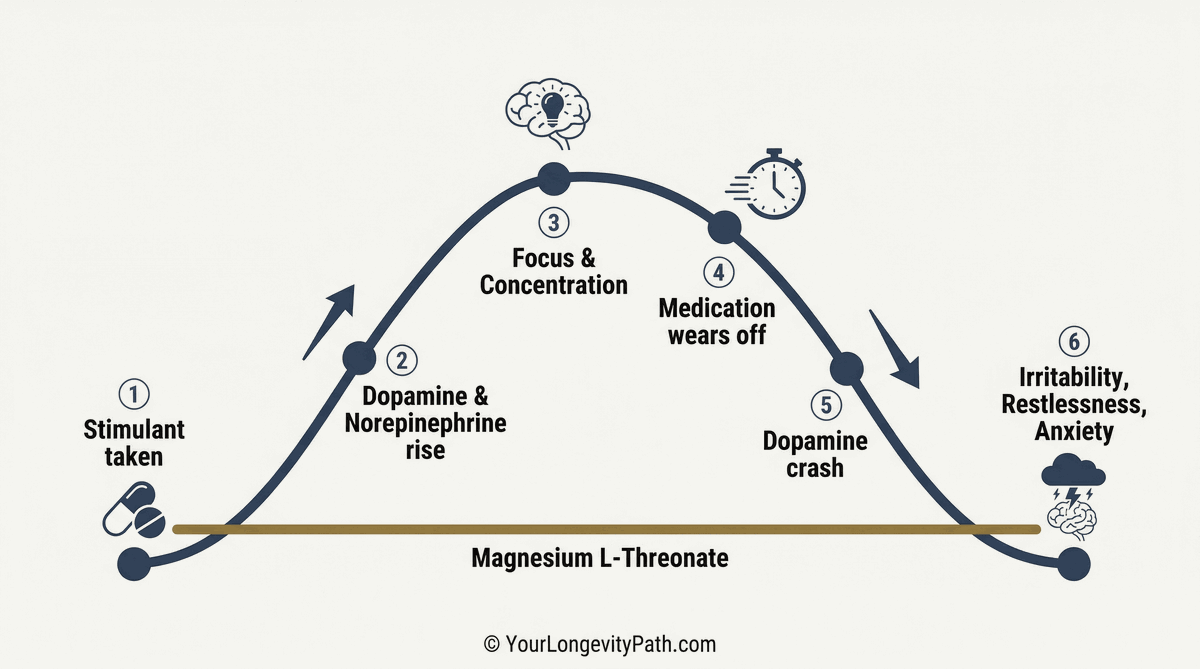 Fig. 4: The typical stimulant rebound cycle in ADHD: After the active phase (steps 1–3), dopamine levels drop sharply (steps 4–6). Magnesium L-threonate (gold baseline) may buffer this crash neurobiologically. © YourLongevityPath.com
Fig. 4: The typical stimulant rebound cycle in ADHD: After the active phase (steps 1–3), dopamine levels drop sharply (steps 4–6). Magnesium L-threonate (gold baseline) may buffer this crash neurobiologically. © YourLongevityPath.com
Clinical Evidence: What the Research Shows
The most direct evidence comes from a 2021 open-label pilot study in 15 adults with ADHD. Over 12 weeks at doses of 1.5 to 2g daily, nearly half the participants met clinical response criteria, defined as a score of 2 or better on the Clinical Global Impressions scale and at least a 25% reduction on the Adult ADHD Self-Report Scale (AISRS). Improvements were most notable in executive function and attention shifting. And critically: the supplement was well tolerated with no serious adverse events (Surman et al., 2021).
Studies like Kozielec & Starobrat-Hermelin (1997) found that up to 72% of children with ADHD had magnesium deficiency. Subsequent research by Mousain-Bosc et al. (2006) showed that supplementing magnesium with vitamin B6 improved performance on the Wisconsin Card Sorting Test, a measure of cognitive flexibility and planning.
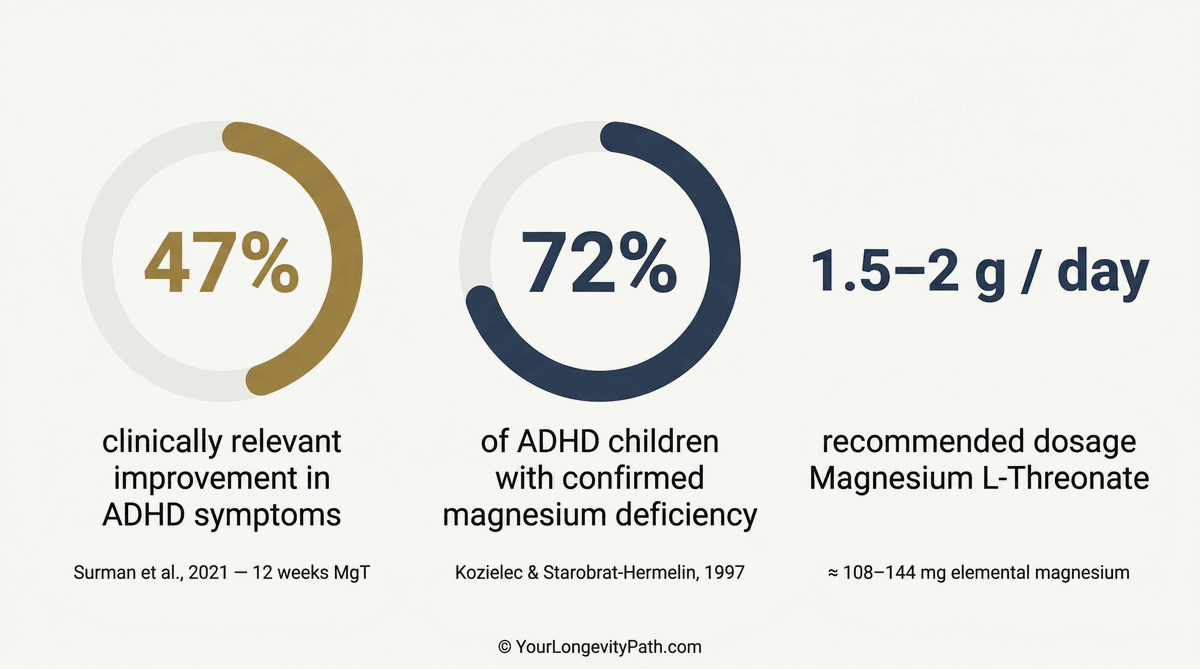 Fig. 3: The key numbers at a glance: Nearly half of adults with ADHD showed clinically relevant improvement, and almost three quarters of children tested had a magnesium deficiency. © YourLongevityPath.com
Fig. 3: The key numbers at a glance: Nearly half of adults with ADHD showed clinically relevant improvement, and almost three quarters of children tested had a magnesium deficiency. © YourLongevityPath.com
None of these studies claim that magnesium L-threonate replaces stimulant medication. That would be neither realistic nor responsible. But the data suggest it can be a meaningful adjunct, particularly for people whose ADHD involves high anxiety, sensory overload, or challenging medication rebound.
How to Use Magnesium L-Threonate Responsibly
If you’re considering this compound alongside ADHD medication, here’s the practical framework:
Talk to your doctor first. This is non-negotiable. Your treating physician needs to know what you’re adding and why. Magnesium can interact with certain medications, particularly those affecting the nervous system, and dosing should be individualized. Since stimulants act on the cardiovascular system and magnesium has a relaxing effect on blood vessels, medical oversight is essential.
Dosing and elemental magnesium: Studies used 1.5 to 2g daily, divided into two doses. Important: 2g of magnesium L-threonate yields only about 144mg of elemental magnesium. It is a targeted brain supplement, not a replacement for your foundational magnesium (like bisglycinate) for muscle and bone health. Think of it as a brain-specific add-on to your mineral strategy.
Starting slowly: In the first few days, some people experience mild headaches, likely due to increased neuronal activity and neuroplasticity as brain magnesium levels rise. Start with 1,000mg in the evening and increase to the full dose after a few days. This allows your brain to adjust gradually.
Timeline: Don’t expect overnight results. This mineral works slowly, rebuilding tissue and stabilizing neural signaling. Most studies ran 12 weeks or longer. Give it at least 4 to 6 weeks before deciding if it’s working.
Rebound specifically: If you’re targeting the rebound effect, the logic would be to take it in the afternoon, building brain levels before medication wears off in the evening. But this is strategic thinking, not established protocol. Your doctor can help you optimize timing.
Quality matters: Not all supplements are equal. Look for products from reputable manufacturers with third-party testing. Some “magnesium L-threonate” products are poorly formulated and won’t deliver the dose claimed on the label. The patented Magtein® formulation has the strongest clinical backing.
The Bigger Picture
ADHD isn’t just a dopamine disorder. It’s a complex dysregulation of multiple neurotransmitter systems, with glutamate excitability playing a central role. Magnesium is one of the body’s master regulators of excitation; it works upstream of dopamine and norepinephrine, not downstream.
This is why L-threonate isn’t a replacement for stimulant medication. It’s a complementary tool that addresses a different piece of the puzzle: the hyperexcitability, sensory overload, and emotional instability that stimulants alone don’t always smooth out.
For some people, it’s transformative. For others, it’s a subtle but real boost: better sleep, fewer afternoon irritability spikes, a slightly easier time staying regulated. Neither outcome should be dismissed. Small, consistent improvements in nervous system stability compound over months and years.
The research is still emerging. But if you have ADHD and you’ve noticed low magnesium on a blood test, or if you struggle with the rebound effect, or if sensory overload and emotional reactivity are your biggest challenges, magnesium L-threonate is worth a serious conversation with your doctor.
For a deeper look at how this compound works on a molecular level and its connection to longevity, read my article Magnesium L-Threonate: How a unique form of magnesium reduces stress and protects your brain. And if you’re wondering how to add new habits without overwhelming yourself, check out One step at a time.
Scientific Sources
Abumaria, N., Yin, B., Zhang, L., Li, X. Y., Chen, T., Descalzi, G., Zhao, L., Ahn, M., Luo, L., Ran, C., Zhuo, M., & Liu, G. (2011). Effects of elevation of brain magnesium on fear conditioning, fear extinction, and synaptic plasticity in the infralimbic prefrontal cortex and lateral amygdala. The Journal of Neuroscience, 31(42), 14871–14881. doi: 10.1523/JNEUROSCI.3782-11.2011
Cheng, J., Liu, A., Shi, M. Y., & Yan, Z. (2017). Disrupted glutamatergic transmission in prefrontal cortex contributes to behavioral abnormality in an animal model of ADHD. Neuropsychopharmacology, 42(10), 2096–2104. doi: 10.1038/npp.2017.30
Effatpanah, M., Rezaei, M., Effatpanah, H., et al. (2019). Magnesium status and attention deficit hyperactivity disorder (ADHD): A meta-analysis. Psychiatry Research, 274, 228–234. doi: 10.1016/j.psychres.2019.02.040
Schmidt, M. E., Kruesi, M. J. P., Elia, J., Borcherding, B. G., Elin, R. J., Hosseini, J. M., McFarlin, K. E., & Hamburger, S. D. (1994). Effect of dextroamphetamine and methylphenidate on calcium and magnesium concentration in hyperactive boys. Psychiatry Research, 54(2), 199–210. doi: 10.1016/0165-1781(94)90006-X
Kozielec, T., & Starobrat-Hermelin, B. (1997). Assessment of magnesium levels in children with attention deficit hyperactivity disorder (ADHD). Magnesium Research, 10(2), 143–148.
Mousain-Bosc, M., Roche, M., Polge, A., Pradal-Prat, D., Rapin, J., & Bali, J. P. (2006). Improvement of neurobehavioral disorders in children supplemented with magnesium-vitamin B6. Magnesium Research, 19(1), 46–52.
Slutsky, I., Abumaria, N., Wu, L. J., Huang, C., Zhang, L., Li, B., Zhao, X., Govindarajan, A., Zhao, M. G., Zhuo, M., Tonegawa, S., & Liu, G. (2010). Enhancement of learning and memory by elevating brain magnesium. Neuron, 65(2), 165–177. doi: 10.1016/j.neuron.2009.12.026
Surman, C. B., Vaudreuil, C., Boland, H., Rhodewalt, L., DiSalvo, M., & Biederman, J. (2021). L-Threonic acid magnesium salt supplementation in ADHD: An open-label pilot study. Journal of Dietary Supplements, 18(2), 119–131. doi: 10.1080/19390211.2020.1731044
Why doesn't regular magnesium work well for ADHD?
Most magnesium forms barely cross the blood-brain barrier. Magnesium L-threonate is the only form proven to significantly raise magnesium levels in the brain.
Can magnesium L-threonate help with ADHD medication rebound?
Studies show it acts as a natural NMDA receptor blocker, dampening the glutamate overstimulation that drives the evening crash after methylphenidate wears off.
How long does magnesium L-threonate take to work?
Clinical studies show initial cognitive improvements after 6 to 12 weeks of regular use. Sleep quality often improves earlier, within the first few weeks.
This article is for informational purposes only and does not replace professional medical advice, diagnosis, or treatment. If you have health concerns, please consult a qualified healthcare professional.